Dr. Manjunath Natarajan, N18243, Dr. Mona Gautam
LIST OF ABBREVIATIONS USED
(in alphabetical order)
- cm – centimetre.
- D –dioptre.
- e- that is.
- m –metre.
- R – Mohindra’s near retinoscopy.
- P.D – out patient department.
- R – Static Retinoscopy.
- S.R – Binocular subjective refraction.
- S.R – Monocular subjective refraction.
- D.T – Worth’s 4 dot test.
- M.T – Post mydriatic test.
- vs –versus.
ABSTRACT
Background:
This study is an attempt to investigate the effectiveness of Mohindra’s near retinoscopy (M.R) technique. The noteworthy feature of this technique being that the results are close to post-cycloplegic retinoscopy, without using cycloplegic drugs. Thus eliminating the use of cycloplegic drugs & their associated side effects.
To avoid the use of cycloplegia in infants and young children and to overcome the difficulty of directing their attention to constantly maintain fixation at a distant target during static retinoscopy (S.R), Mohindracame up with a new method of performing retinoscopy which has been named Mohindra’s near retinoscopy1.The technique is particularly valuable for refracting infants and young children who would otherwise require cycloplegia, and it may be an effective clinicalmethod for the correction of night myopia and related accommodation anomalies in adults2.
Thusit is a promising method through which efficient refractive error screening and evaluation could be performed. Hence it needs further evaluation & understanding.
Although a few studies have used the near retinoscopy technique of Mohindra, none have thus far have tried to scrutinize its relation to subjective acceptance or to static retinoscopy.
Objectives:
1)Correlation of static retinoscopy with monocular and binocular subjective correction.
2) Correlation of Mohindra’s retinoscopy with monocular and binocular subjective correction.
Methods:
Study Design:One and a half year, prospective observational non-randomized study using purposive sampling.
Study sample:
Sample size is 100 eyes.
Methodology:
A prospective observational study using purposive sampling was conducted to find a correlation between two methods of retinoscopy namely static retinoscopy (S.R) &Mohindra’s near retinoscopy (M.R). These two values were then correlated with two methods of subjective refraction namely monocular subjective refraction (M.S.R)& binocular subjective refraction (B.S.R).
After obtaining their consent, patients eligible to be included in the study with respect to inclusion & exclusion criteria were made to undergo routine evaluation protocol for refractive error, which along with ocular examination, also includes static retinoscopy (S.R) with monocular subjective refraction (M.S.R) & in addition, were made to undergo Mohindra’s near retinoscopy (M.R) & binocular subjective refraction (B.S.R).
Estimates of refractive error by S.R & M.R and also the acceptance by both M.S.R & B.S.R were recorded and converted to spherical equivalents & were subjected to statistical analysis to find a correlation between them.
Results:
There is a very good correlation between all the variables considered for the study.
Pearson’s correlation between S.R & M.R and between M.S.R & B.S.R indicate a good correlation.
The Bland-Altman plot of S.R vs M.R & M.S.R vs B.S.R both show a very low bias estimate & a good agreement between the values.
The results of Passing and Bablok regression analysis shows a plot with very good agreement between S.R & M.R and between B.S.R & M.S.R values & also the plot between these variables respectively show all values lie within allowable bias limits.
Interpretation & Conclusion:
All the four variables (i.e. S.R, M.R, M.S.R, B.S.R) considered for the study were found to have a good correlation & agreement with each other. Both retinoscopy methods showed close correlation with each other & with both thesubjective acceptance methods.
The results in this study show that there is nosignificant difference between near retinoscopy and subjective refraction, which supports the results found by Mohindra1.
Both S.R & M.R techniques have good correlation with binocular refraction. M.R had a closer correlation with B.S.R than M.S.R. S.R had a closer correlation with M.S.R than B.S.R.
This is the first study to try to find a correlation between these variables using refractive errors of such magnitude.
Keywords:Retinoscopy; Ocular refraction.
INTRODUCTION
Ocular refraction refers to the refraction of light effected by the media of the eye.When light rays meet the interface separating two transparent media of different optical densities, some of the light gets reflected but most of it gets transmitted through the medium.
The process of transmission of light through a new medium whereby the incident ray of light undergoes a change in its velocity due to the difference in density in the second media as compared to the first istermed refraction3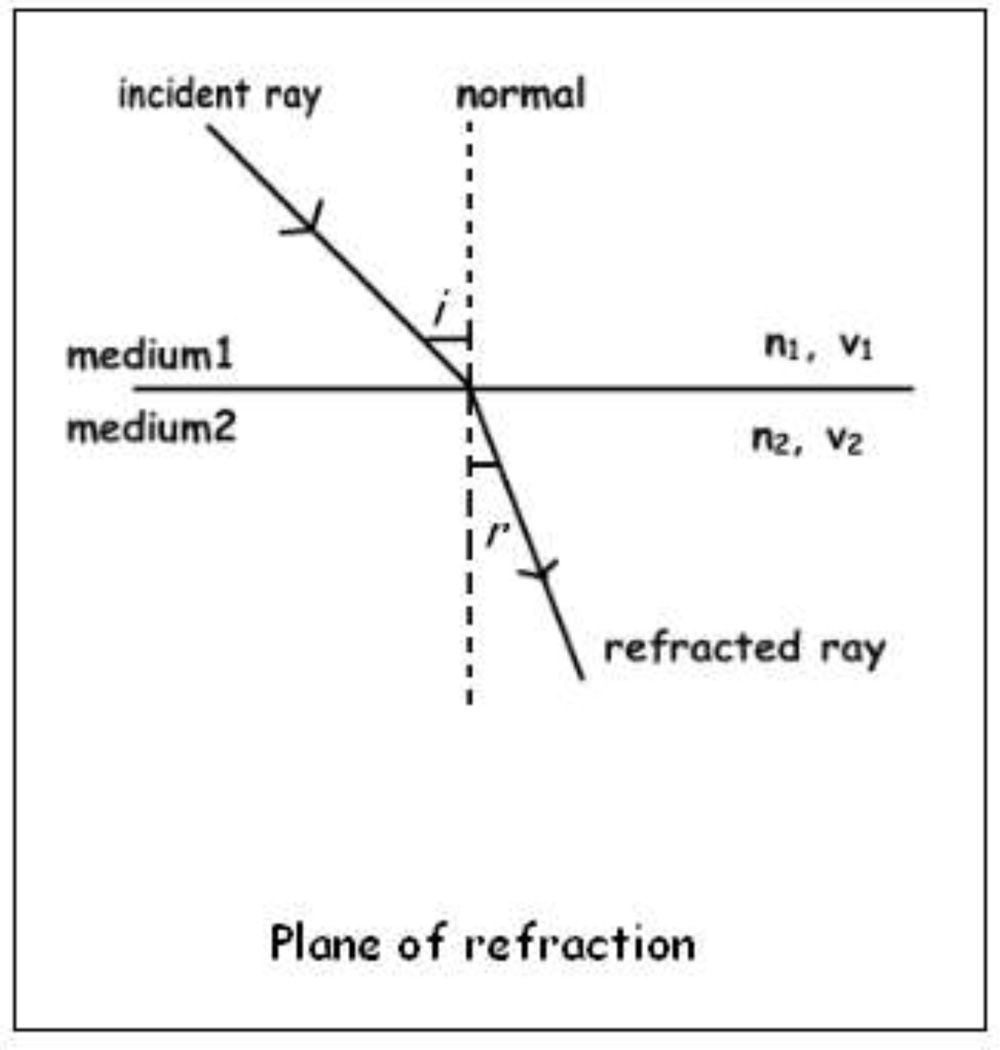
Fig.1. Refraction of light occurring when a ray of light travelling from medium 1 of refractive index n1 with velocity v1, passes on to medium 2 with a refractive index n2 and velocity v2. The angle of incidence being “i” and the angle of refraction being “r”.
The phenomenon of refraction makes image formationpossible by the eye by bringing the incident light rays to focus on the retina. The eye is an optical system with a positivepower of about 58 to 68 D.It has two main refractive elements, the cornea and the lens. The anterior surface of the cornea is in contact with air, hence light rays incident on it will encounter a greater differencein refractive index at thisinterface. Hence the cornea refractsthese rays maximally and bears most of therefractive power of the eye3.
The eye is like an optical instrument. It is well compared toa camera with the retina acting as a unique kind of ‘film’. The focusing system of eye is composed of several refracting structures with different refractive indices which include:
| REFRACTIVE MEDIA | REFRACTIVE INDICES |
| The cornea | 1.37 |
| The aqueous humour | 1.33 |
| The crystalline lens | 1.42 |
| The vitreous humour | 1.33 |
Table.1. The refractive media of the eye with their respective refractive indices.
Schematic eye
The schematic eye represents a simplified, mathematical modelof the optical system of the eye which facilitates the understanding of geometric optics with relation to the eye.
Many such models, combining the sciences of optics, physics, mathematics and ophthalmology have been proposed in literature, one such model which both accurate and simple to understand is the Gullstrand’s simplified schematic eye model or the Gullstrand-Emsley model3.
Emsley’s schematic reduced eye has the following charecteristics3:
• Power of 60 D.
• An index of refraction of 1.33.
• Radius of curvature of 5.55 mm.
• The refracting surface was situated 1.66 mm behind the schematic eye’s cornea.
• Anterior and posterior focal lengths of –16.67 mm and +22.22 mm respectively.
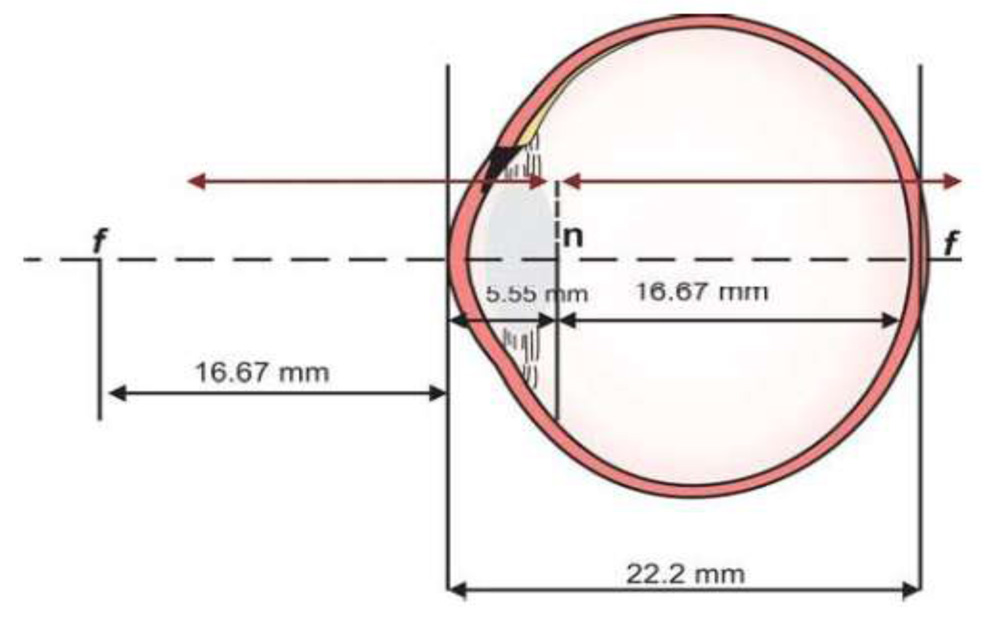
Fig. 2. The schematic eye depicting the cardinal points
According to the schematic eye, the incident parallel light rays come to a focus at the posterior focal point, which in the human eye happens to be on the retina. Thus, an eye in which incident parallel light rays come to a focus on the retina with the accommodation at rest, isemmetropic(normal refractive system of the eye).
An eye in which the incident parallel light rays come to a focus either infront of or behind the retina with the accommodation at rest, isametropic3.
The types of ametropia or refractive errors3 are:
• Myopia is therefractive error in which the rays of incident light from infinityare focused in front of the retina, in an unaccommodated state. Myopia is corrected using concave/ diverging/ minus lenses.
• Hyperopia or hypermetropia is the refractive error in which the rays of incident light from infinity are focused behind the retina, in an unaccommodated state.Hypermetropia is corrected using convex/ converging/ plus lenses.
• Astigmatism is that state of refractive error where in anunaccommodated state, differences in the curvatures of therefracting media of the eye can result in the formation ofimages at two focal points.Astigmatism is corrected using cylindrical lenses which could be concave or convex of the respective power and axis.
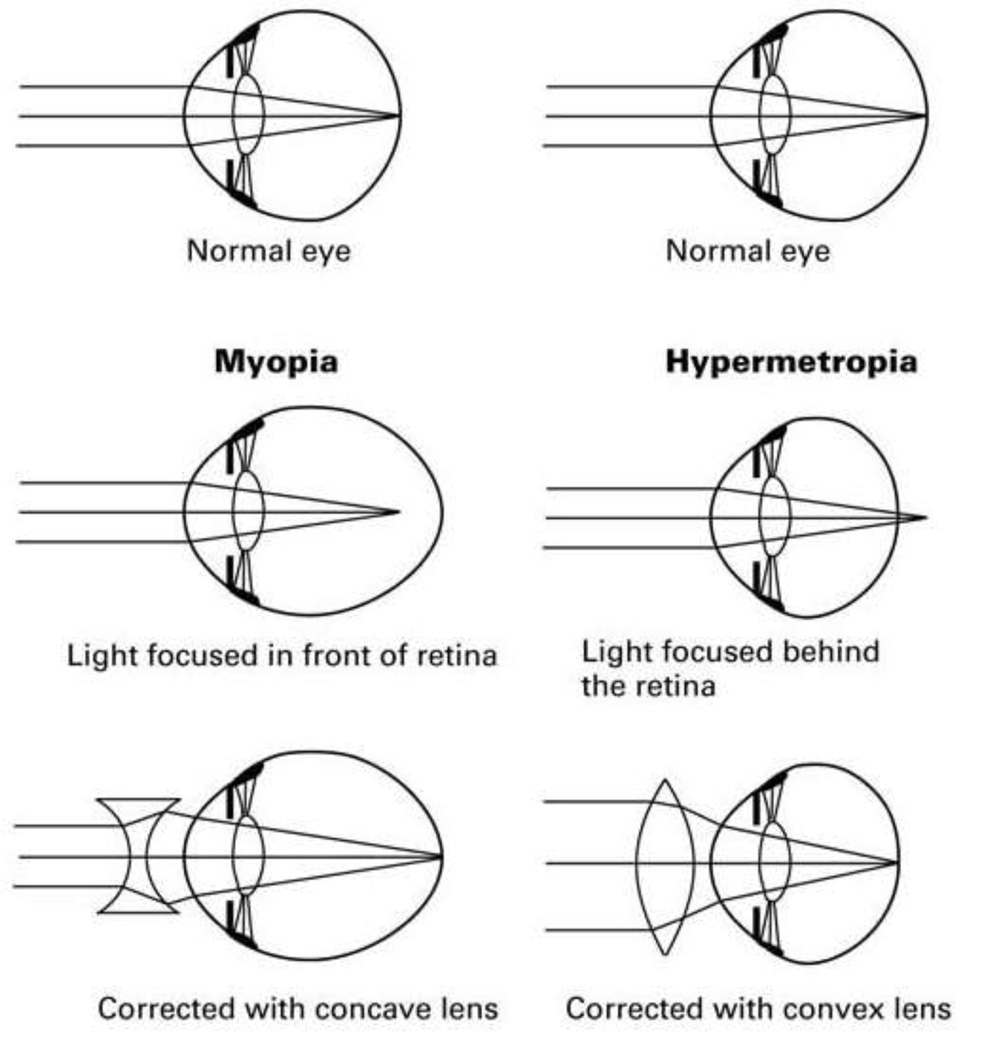 Fig. 3. Ray diagrams showing refraction of light in myopic and hypermetropic eyes, depicting refraction of light through the refractive media of the eye, in the uncorrected and corrected states.
Fig. 3. Ray diagrams showing refraction of light in myopic and hypermetropic eyes, depicting refraction of light through the refractive media of the eye, in the uncorrected and corrected states.
In order to treat the conditions with the prescription of appropriate power spectacle lenses, we need to first determine the magnitude of the refractive error of that eye. This can be done by either objective methods, known as objective refraction or by using subjective methods, known as subjective refraction.
Objective refraction is the determination of the refractive error of the eye without any input from the patient. These are essential techniques by which we can assess the refractive status of the eye. These give a good starting point for the subjective refraction of patients. The most common tools for objective estimation of refractive status are:
• Retinoscopy,
• Auto-refraction.
Of these methods, retinoscopy has the status of gold standard4,5.
In subjective refraction, the examiner is guided by the patient’s response to the changes in the appearance of observed targets as the power of the lenses before the patient’s eye is altered. This determines the final power of the spectacles that is prescribed to the patient, optimizing his visual needs. It is important to note that irrespective of how good the quality of objective refraction may be, the final prescription is based solely on subjective refraction. This holds true in all patients except in patients who are uncooperative due to various causes, in whom the prescription is given based on the objective refraction.
Retinoscopy
Retinoscopy is the gold standard method of objective refraction. The retinoscope is an instrument used to project a beam of light into the patient’s eye and estimate the refractive error of that eye by the appearanceof the arising reflexes.
History and evolution of retinoscopy.
The principle of objective refraction was discovered in 1859, when Sir William Bowman noticed a peculiar light and shadow reflex in an astigmatic eye when moving an ophthalmoscope beam across the pupil. After this discovery Bowman made use of the reflex in diagnosing astigmatism. In 1873, the French ophthalmologist Cuignet introduced the clinical use of retinoscopy. In 1878,Landolt made the first attempts to explain the underlying optical principles of retinoscopy. The theory was updated by Parent in 1881, and he also introduced the term “retinoscopie” (vision of the retina) and later “skiascopie” (vision of shadows). In addition to static retinoscopy there also exist the technique of dynamic retinoscopy which objectively estimates accommodation lag4.
Mohindra’s near retinoscopy investigated in this study is a distinct entity not to be confused with either static or dynamic retinoscopy. In her paper in 1977, Mohindra found near retinoscopy readings to be close to post-cycloplegic retinoscopy1, therefore avoiding cycloplegia& side effects of cycloplegics.
Hence this is a promising method of objective refraction, offering several advantages to both patients and ophthalmologists/optometrists compared to conventional refractive error screening & correction.
Not much research has been done in this area since Mohindra’s paper in 1977. Although a few studies have made useof the near retinoscopy technique of Mohindra, none thus far have tried to scrutinize its relation to subjective acceptance or to static retinoscopy.
Hence an attempt has been made to test its efficacy by finding a correlation between Mohindra’s near retinoscopy(M.R) & static retinoscopy(S.R), then comparing the values to subjective refraction, tested using the monocular subjective refraction (M.S.R) & binocular subjective refraction (B.S.R).
Salient features of objective refraction using aretinoscope
Apart from a more accurate result, the advantages of retinoscopy over auto-refraction are that it can provide information about the ocular health and function.
This includes:
• Detection of media opacities & their localization,
• Accommodative status can be assessed using dynamic retinoscopy throughout the procedure of retinoscopy. This allows the examiner to identify abnormalities such as pseudomyopia.
Several studies comparing autorefractor to retinoscopy have been carried out a few of which state that although auto refraction provides a fast and reliable measurement in many cases it often yields a more myopic result and large differences occasionally occur6.
Non-cycloplegic auto-refraction underestimates hyperopia to a clinically unacceptable degree in children. Retinoscopy is much more likely to yield a clinically acceptable measure of hyperopia7.
Auto-refraction will give inaccurate or no readings at all in a substantial number of patients with small pupils, media opacities, irregular corneas &nystagmus.Retinoscopy will often give a better result4,5.
Retinoscope also offers several advantages such as:
1. Portable,
2. Lower cost,
3. Easy to use,
4. Can be used in remote areas without a continuous power supply,
5.Can be used in a variety of patient postures, especially useful in patients unable to sit erect or position themselves on the autorefractometers,
6. Non-invasive and Non-contactmethod.
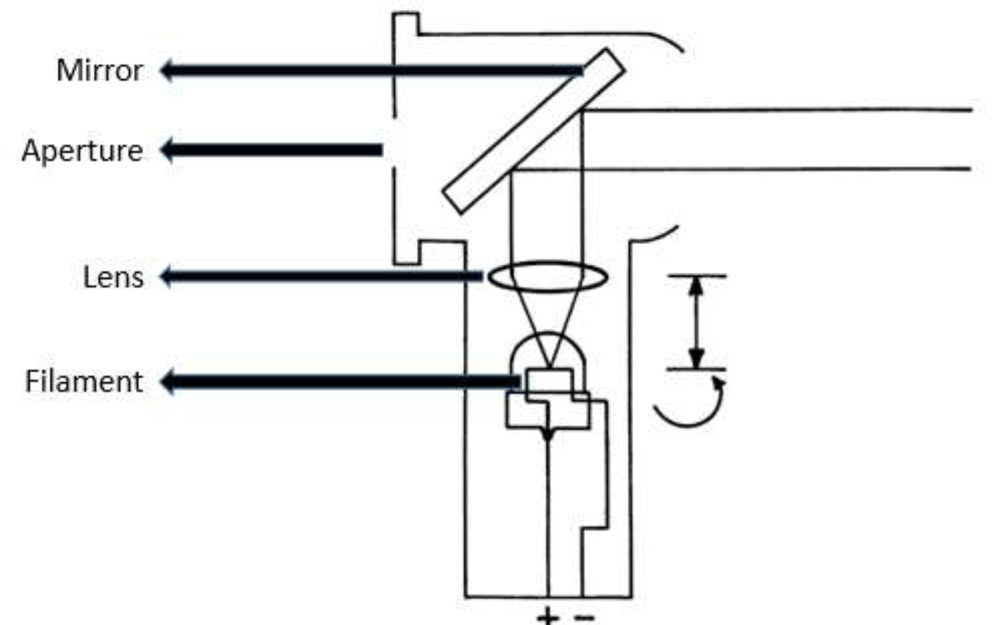 Fig. 4.Diagrammatic cross-section of a streak retinoscope.
Fig. 4.Diagrammatic cross-section of a streak retinoscope.
In fig. 4, light from the filament passes through the lens to the mirror, where it is reflected toward the patient. The examiner views through the aperture behind the mirror. The arrows on the right represent the two controllable functions. The curved arrow indicates that the bulb may be rotated. The vertical arrow indicates that the vergence of the light rays may be altered by changing the filament to lens distance. The filament is shown at the focal length of the lens so that parallel light rays emerge.
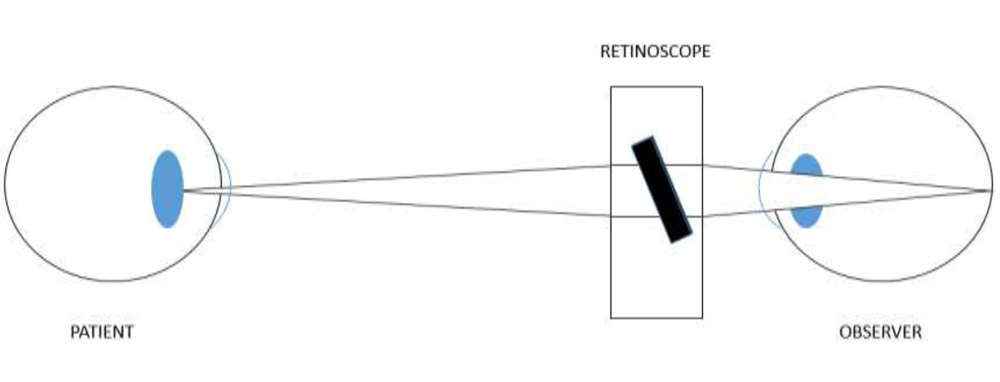 Fig. 5. Observation system: light path from patient’s pupil, through mirror, to observer ‘s retina.
Fig. 5. Observation system: light path from patient’s pupil, through mirror, to observer ‘s retina.
Working of a retinoscope
Retinoscopes can be either streak or spot retinoscope depending on the shape of light they project. Most retinoscopes in current use employ the streak projection system developed by Copeland. The illuminationis provided by a bulb with a straight filament that forms a streak8.
The filament light source can be moved in relation to a convex lens in the system giving rise to configurations in which retinoscopy can be done, namely:
1) Plano mirror setting: If the light is slightly divergent, it appears to come from a point behind theretinoscope, as if the light were reflected off a flat mirror as in fig. 6.
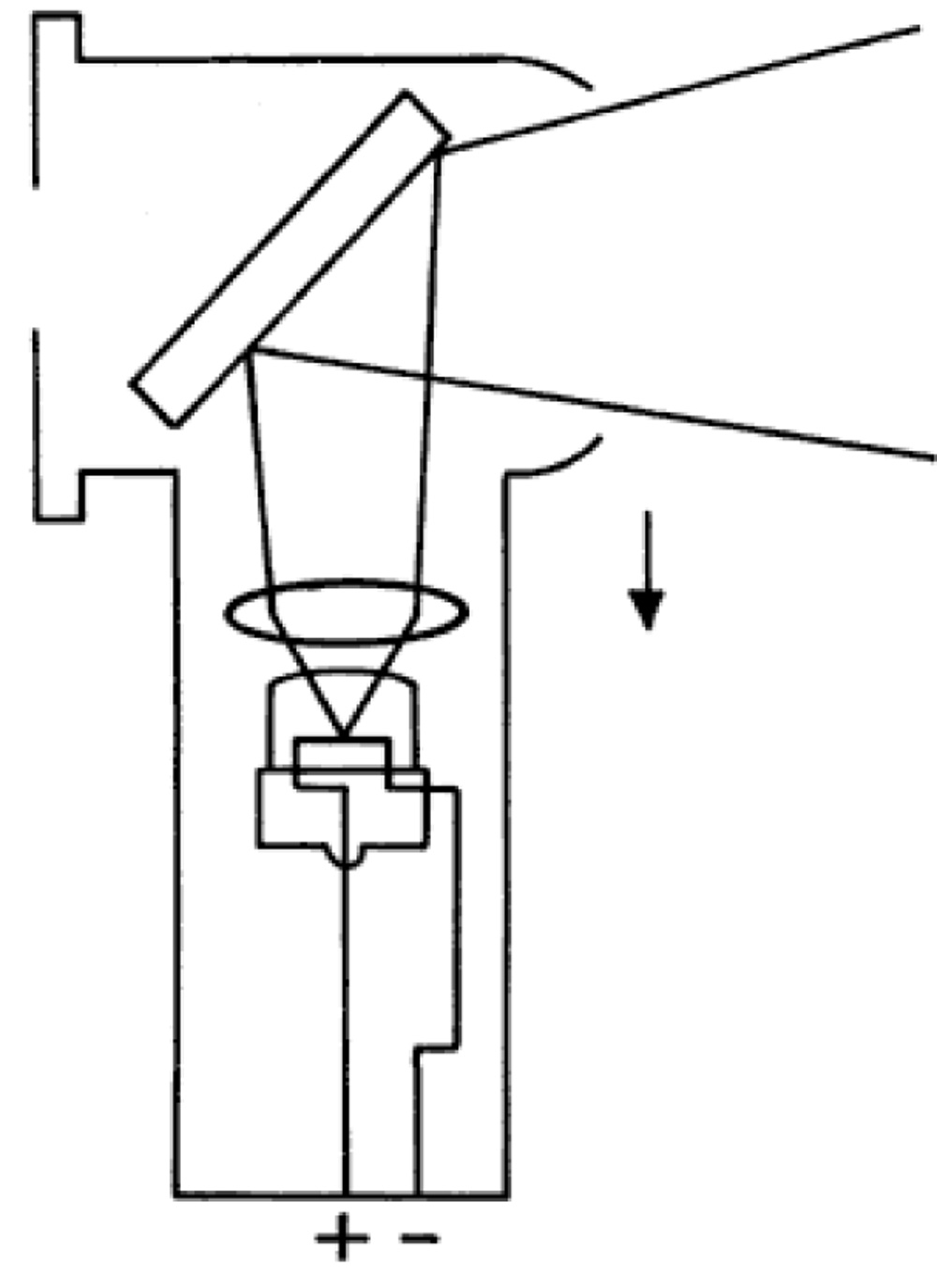 Fig. 6.The divergent beam of light emitted as a result of the optical effect of moving the lens closer to the filament8.
Fig. 6.The divergent beam of light emitted as a result of the optical effect of moving the lens closer to the filament8.
2) Concave mirror setting: When the distance between the convex lens and the filament is increased by moving the sleeve on the handle, convergent light is emitted. In this situation,the image of the filament appears between the examiner and the patient, as if the light were reflected off a concave mirror as in fig. 7.
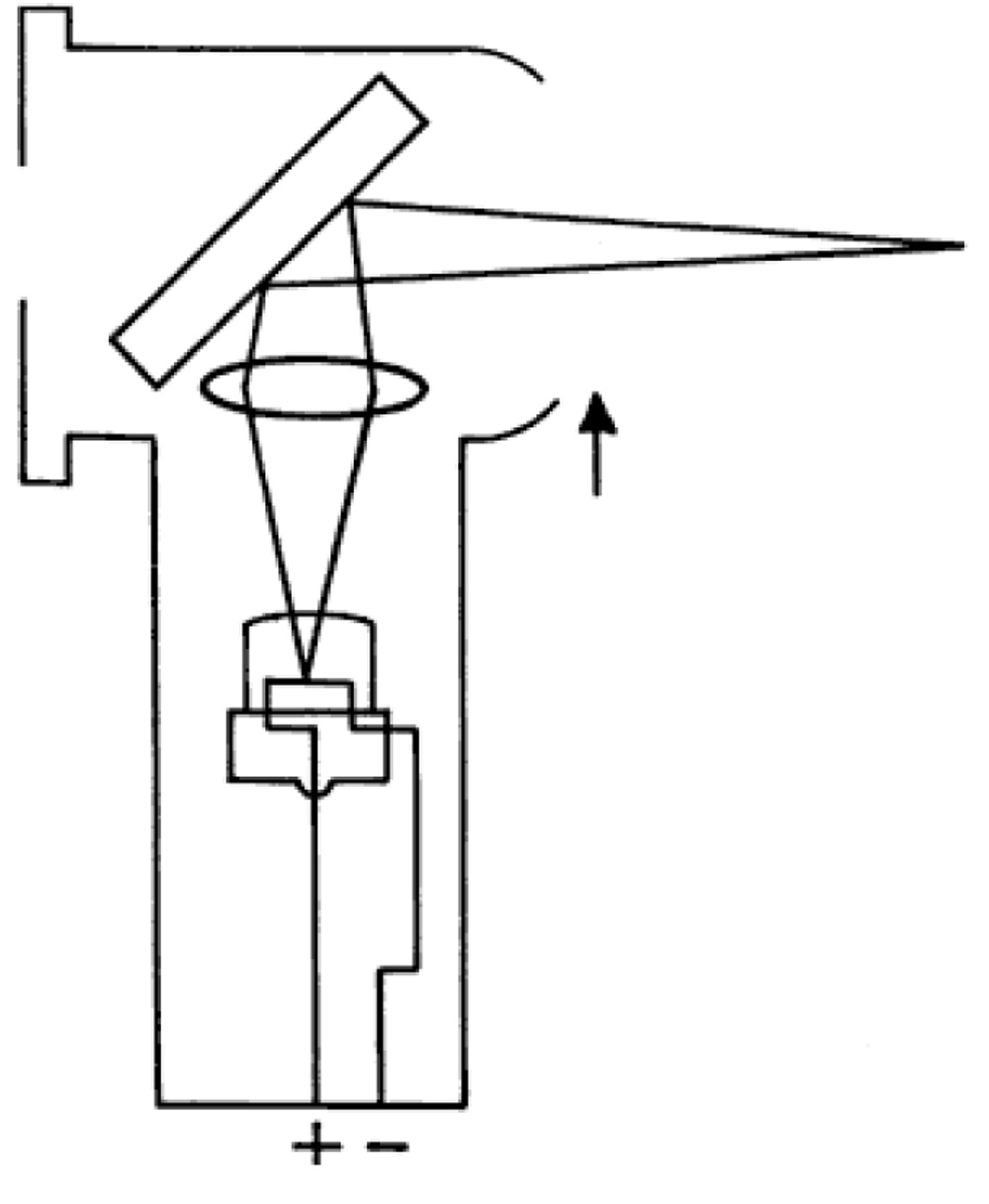 Fig. 7. The convergent beam of light emitted as a result of the optical effect of moving the lens farther away from the filament8.
Fig. 7. The convergent beam of light emitted as a result of the optical effect of moving the lens farther away from the filament8.
Calibration of a retinoscope
If the condensing lens is moved from the lowest (plane mirror) position upwards along the shaft of the instrument, an intermediate position is reached at which a focused image of the retinoscope bulb filament falls on the patient’s eye (or cheek).
The effect here is that of a concave mirror of focal length equalling the retinoscope–patient distance and is of no value for retinoscopy as the image of the light source is coincident with the patient’s eye9.
Now if the retinoscope’s condensing lens is moved a short distance back down the shaft of the retinoscope, the ‘plane mirror effect’ is regained but with a much brighter illumination than that obtained with the condensing lens at its lowest position9.
The retinoscope is now acting as a concave mirror of focal length slightly exceeding the observer–patient distance.
The advantages of this position are9:
1) The plane mirror effect which most observers prefer is retained.
2) A bright retinoscopy reflex is achieved which make retinoscopy easier especially in cases of small pupils.
In the Heine beta 200 retinoscope used in this study, this effect was easily attained using the ParaStop technology, so that the sleeve position can easily be set to achieve the plane-mirror effect i.e. the unique ParaStop technology enables us to achieve the “Plano-mirror” setting easily.

Fig. 8.The ParaStop system used to achieveplano mirror calibration.
Retinoscopes of different types can have different sleeve positions for the plano mirror setting. For example, the original Copeland retinoscopeis in plano position with the sleeve up; the Welch Allyn instrument is in plano position with the sleeve down, same as the Heine beta 200 retinoscope used in this study. The axis of the streak can be altered by rotating the sleeve to enable estimation of astigmatism8.
Retinoscopy is usually performed using the plano mirror setting. All retinoscopy measurements in the current study have been recorded in the plano mirror setting.
Stages of the retinoscopy reflex
• The illumination stage – The retinoscope’slight is directed into the patient’s eye to illuminate the retina8.
• The reflex stage – An image of the illuminated retina is formed at the patient’s far-point8.
• The projection stage – The image at the patient’s far-point islocated by moving the illumination across the fundus and noting the behaviour of the luminous reflexseen by the observer in the patient’s pupil8.
During retinoscopy the patient’s far point is altered by placing correcting lenses of different power in front of the patient’s eye so as to bring the far point at the retinoscope’s peephole.
When this is accomplished, the light reflex fills the patient’s entire pupil (neutralization).
The power of the correcting lensneutralizing the reflex helps to determine the patient’s refractive error. The dioptric equivalent of the working distance is subtracted from the power of the correcting lens to make the patient’s retina conjugate with optical infinity.
Nature of reflexes in retinoscopy:
• With movement: here the light reflex moves with the direction of movement of the retinoscope beam & is observed when the far point is behind the examiner i.e the patient’s is more hypermetropic than the working distance equivalent diopteric power. Here the light rays come to a focus behind the examiner.

Fig. 9.Behaviour of the reflex during retinoscopy of a hypermetrope.
• Against movement: here the light reflex moves against the direction of movement of the retinoscope beam & is observed when the far point is between the patient & the examiner i.e the patient is more myopic than the working distance equivalent diopteric power. Here the light rays would have converged to a point & later diverged again.

Fig. 10.Behaviour of the reflex during retinoscopy of a myope.
• Theneutral pointof retinoscopy is reached when the patient’s far-point coincides with the observer’s nodal point. No movement of the reflex can be discerned in the patient’s pupil. The observer sees a diffuse bright red reflex which fills the patient’s pupil. This is because at this stage the movement of the reflex is infinitely rapid.

Fig. 11.Behaviour of the retinoscopy reflex during neutralization.
Characteristics of reflexes observed during retinoscopy
• Speed. The reflex seen in the pupil moves slowest when the far point is distant from the examiner/peephole of the retinoscopei.e the point of neutralization is far away. As the far point is moved toward the peephole, the speed of the reflex increases. In other words, large refractive errors have a slow-moving reflex, whereas small errors have a fast reflex9.
• Brilliance. The reflex is dull when the far point is distant from the examiner; it becomes brighter as neutrality is approached. Against reflexes are usually dimmer than with reflexes9.
• Width. When the far point is distant from the examiner, the streak is narrow. As the far point is moved closer to the examiner, the streak broadens and, at neutrality, fills the entire pupil9.
Determination of the axis of astigmatism
• Break. A break is seen when the streak is not oriented parallel to one of the principal meridians. The reflex streak in the pupil is not aligned with the streak projected on the iris and surface of the eye, and the line appears broken. The break disappears (i.e. the line appears continuous) when the projected streak is rotated to the correct axis9.
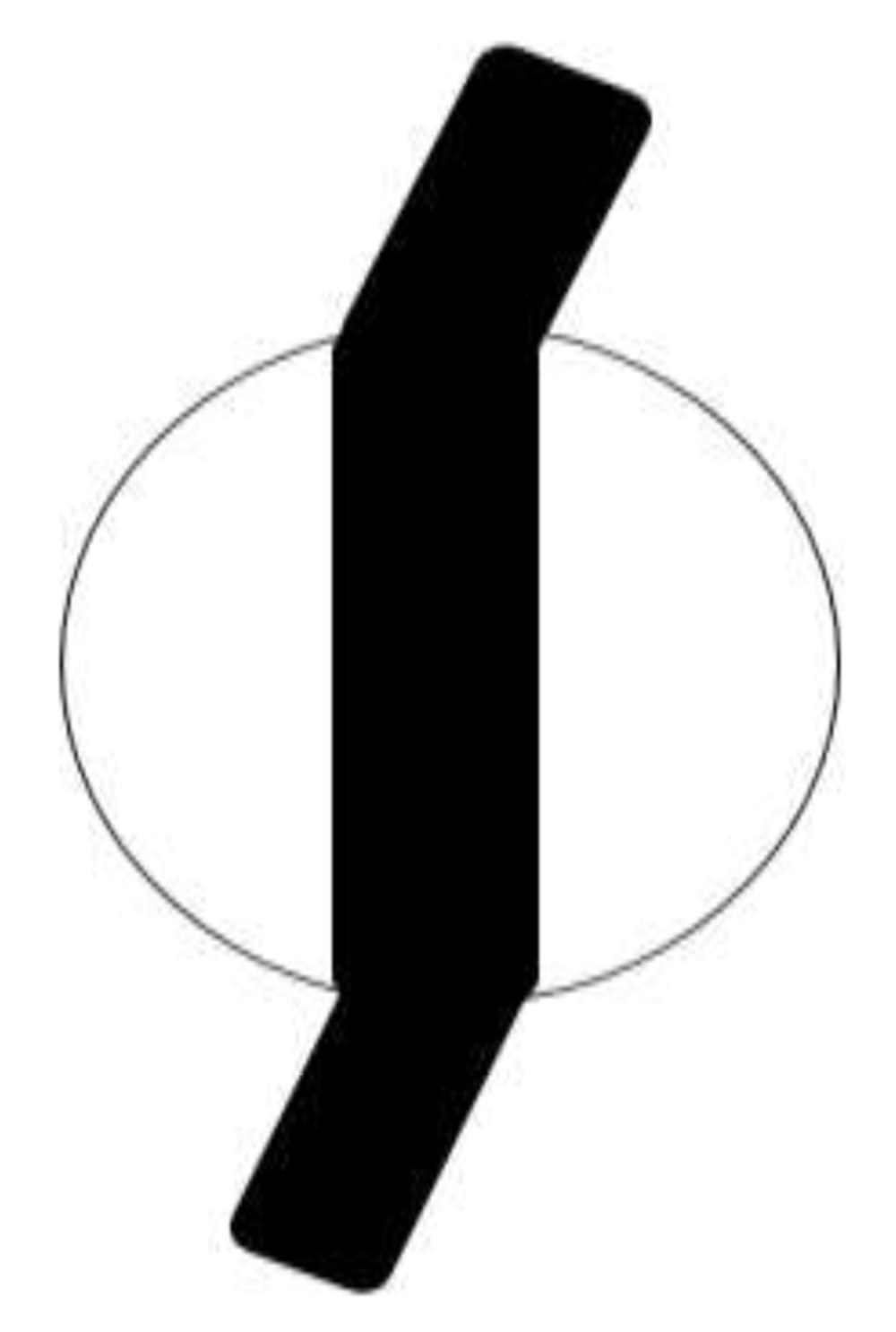
FIG. 12.“Break” in the retinoscopy reflex.
• Skew. Skew (oblique motion of the streak reflex) may be used to refine the axis in small cylinders. If the retinoscope streak is off-axis, it will move in a slightly different direction from the pupillary reflex. The reflex and streak move in the same direction when the streak is aligned with one of the principal meridians.
• Width. The width of the reflex in the pupil varies as it is rotated around the correct axis. The reflex appears narrowest when the streak aligns with the axis.
 FIG. 13. The narrowed reflex seen when the retinoscope beam is aligned along the axis of astigmatism.
FIG. 13. The narrowed reflex seen when the retinoscope beam is aligned along the axis of astigmatism.
• Intensity. The intensity of the reflex is brighter when the streak is on the correct axis.
Procedure of cycloplegic refraction.
After cycloplegic drops are applied, patients are made to wait tillcycloplegia has beenestablished. Then refractive error estimation is performed.
The cycloplegic effects of the commonly used drugs can last for several days as shown in table 109. After the cycloplegic effects wear off, the patient needs to re-visit the doctor for a Post-Mydriatic Test (P.M.T.), wherein the patient is made to undergo subjective refraction based on refractive error estimated& the final prescription given.
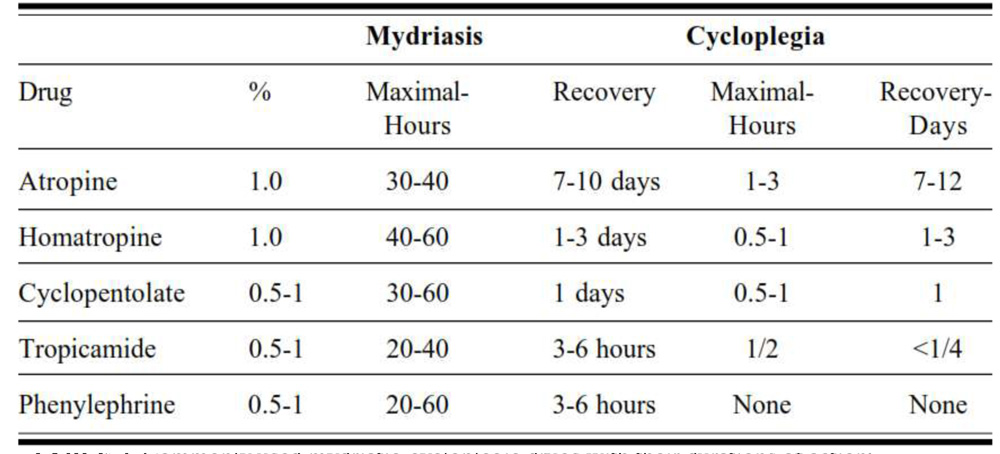 TABLE 2. Commonly used mydriatic-cycloplegic drugs with their durations of action9.
TABLE 2. Commonly used mydriatic-cycloplegic drugs with their durations of action9.
During this period between the first visit & P.M.T the patient willhave blurred vision due to poor accommodation & has to manage without corrective visual aid and he/she will be less able to performtasks which require good near visual acuity. Daily wage labourers, people belonging to the salaried working class & students are likely to suffer from a loss of productivity in this duration.
 Fig.14. Flowchart of the process of cycloplegic refraction using static retinoscopy, the clock symbols denote time delays during this process.
Fig.14. Flowchart of the process of cycloplegic refraction using static retinoscopy, the clock symbols denote time delays during this process.
The demerits of this process are:
1) Cycloplegia makes even routine activities like walking, driving, reading demanding. So is quite uncomfortable & distressing to patients
2) The high cost of cycloplegic eye drops whenconducting mass screening camps or in health care facilities with good patient inflow.
3) Post cycloplegiathe patient will have blurred vision for atleast a day, causing loss of productivity especially so in case of students, salaried working class & the daily wage labourers who are solely reliant on daily wages for their livelihood.
4) The risk of systemic & ocular side effects including allergies due to cycloplegics (table 3).
5) The patient needs to again visit the doctor for P.M.T & final prescription, patient’s Productivity& wages are lost. The doctors are also burdened with seeing same patient twiceadding to their time constraints
The commonly used mydriaticcycloplegic drugs areanticholinergics such as atropine/cyclopentolate/tropicamide.
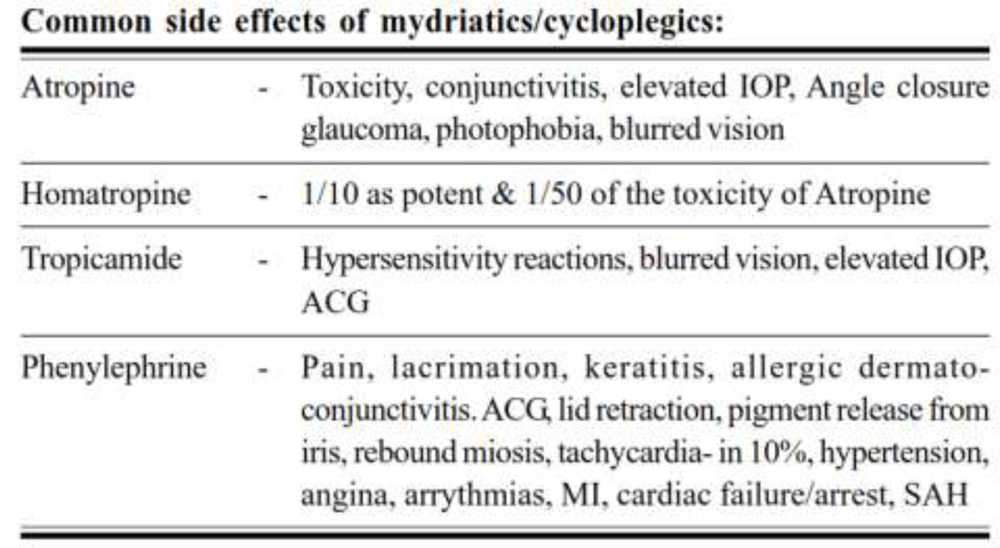 Table.3. Common side-effects of mydriatic-cycloplegic drugs9.
Table.3. Common side-effects of mydriatic-cycloplegic drugs9.
To overcome these disadvantages Mohindra devised a method of near retinoscopy in which the fixation target is the non-accommodative stimulus of the light of the retinoscope itself2. This technique has been shown to produce results close to post-cycloplegic retinoscopy1.
The advantages of Mohindra’sretinoscopy over static retinoscopy are:
1) Avoids cycloplegia, its disadvantages& side-effects listed above.
2) The process of correcting refractive errors is streamlined with minimal use of the resources of both patients &ophthalmlogist/optometrist.
• Patient- less waiting time, no blurred vision, no loss of working hours, no discomfort of cycloplegia& no drug side effects.
• Ophthalmlogist/optometrist-single visit completes the treatment process, more patients screened per day & does not need cycloplegia.
Hence this study has been taken up to find out correlation between static &Mohindra’s retinoscopy with mono & binocular subjective refraction.
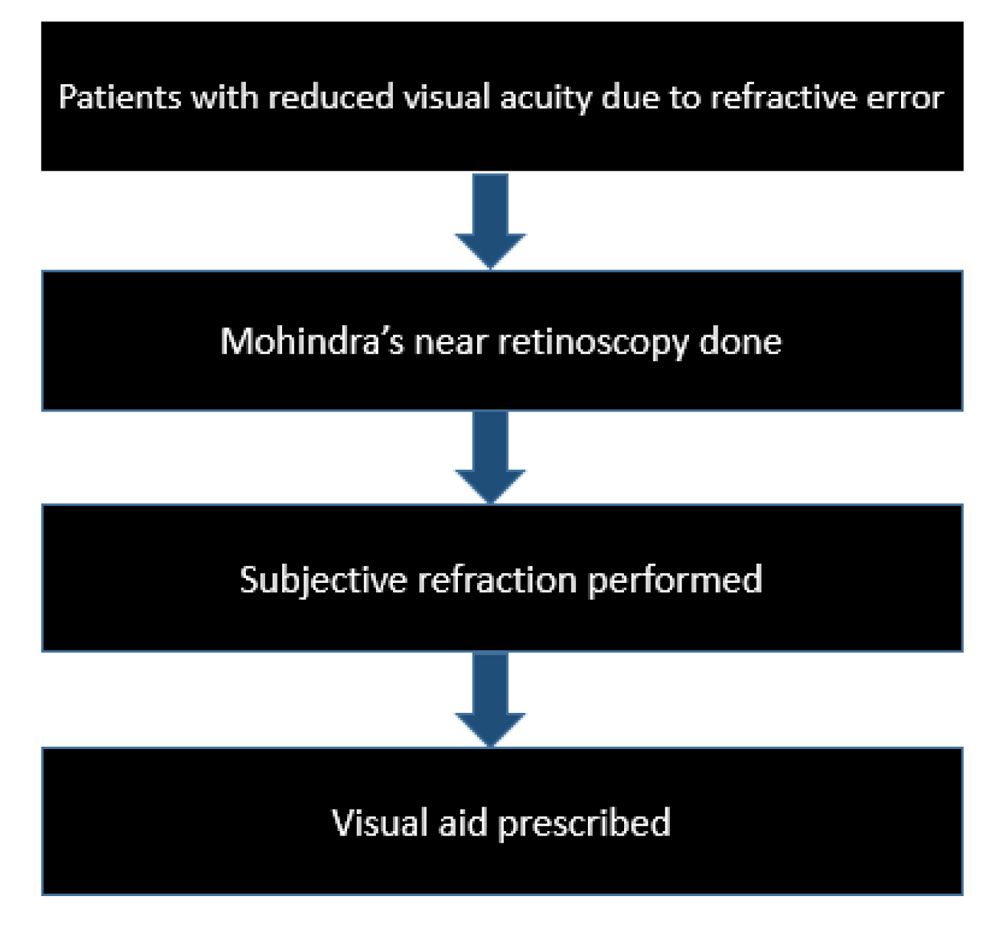
Fig. 15.Flowchart of the process of refractive error correction usingMohindra’s technique
In this study, we have attempted to find a correlation of Monocular subjective refraction (M.S.R)with both static &Mohindra’sretinoscopy resultsas M.S.R is the most commonly used technique.The procedure of Monocular subjective refraction has been explained under methodology of the study.
In Binocular subjective refraction (B.S.R) the patient has both of his eyes open& hence reflex mydriasis in the tested eye as seen in monocular refraction is avoided, therefore a decreased incidence of spherical errors & aberrations. Accommodation is stable & more relaxed.Even though not commonly used, B.S.R is a superior method of refraction as compared to M.S.R, hence we have attempted to find a correlation between binocular refraction& retinoscopy. The procedure of B.S.R has been explained under methodology of the study.
To ensure binocularity while performing the B.S.R,Worth’s four dot test(W.D.T) has been used.The W.D.T is a test of sensory fusion.

Fig. 16.The Worth’s four dot test, showing one red, two green and one white light.
Procedure of Worth’s four dot test10
• The test uses red-green glasses, the red lens is placed in front ofthe right eye and the green lens in front of the left.
• Atarget consisting of 4 dots: 1 red, 2 green, and 1 white is shown to the patient from 6 meters distance.
• The red lens blocks the green light, and the green lens blocks the red light, so the red and green dots are each seen by only 1 eye. The white dot is the only feature seen by both eyes, but it is seen in colour rivalry in a patient with fusion ability.
• The testshould be administered in good ambient light so that peripheral features in the room can stimulate motor fusion. The patient then reports thenumber of dots seen:
1. Seeing 2 red dots indicates a suppression scotoma in the left eye & 2 green dots indicate a suppression scotoma in the right eye.
2. Seeing 3 dots indicates a suppression scotoma in the right eye.
3. Seeing 4 dots indicates that there is some degree of sensory fusion and that the patient has normal retinal correspondence(if there is no manifest strabismus) or harmoniousanomalous retinal correspondence (if there is manifest strabismus).
4. If there is a scotoma, the perception of 4 dots indicates that the scotoma must be smaller than the test target.
5. Seeing 5 dots is a diplopia response. The patient has manifest strabismus withoutsuppression or anomalous retinal correspondence.
Spherical endpoint
The endpoint of subjective refraction should be the maximum amount of positive powerproviding the best visual acuity with accommodation relaxed. When this occurs the circle ofleast confusion is on the retina and the far point of the eye at infinity.
Sometimes the spherical endpoint can be somewhat uncertain, and it is necessary to use a different method to confirm it. The duochrome test, has been used for this purpose in this test9,10. This test uses chromatic aberration to determine the spherical endpoint. As green light is refracted stronger than red the green image on the retina will be slightly in front of thered.

Fig. 17.The duochrome test.
Interpreting the duochrome test:
• If the patient reports that the symbols on the red half of the board are clearest it means that the red image is closest to the retina and the patient is myopic, hence more negative power should be added.
• If the green image is the clearest, the patient is hypermetropic, hence positive power is added,
• When both images are equally clear the endpoint is obtained.
Determination of cylindrical correction using a cross-cylinder
The cross-cylinder is a type of toric lens used during refraction. Its use was popularised by Edward Jackson (1893–1929) and it is often referred to as ‘Jackson’s cross-cylinder’.
The cross-cylinder is a sphero-cylindrical lens in which the power of the cylinder is twice the power of the sphere and of the opposite sign.
Clinically the cross-cylinder is used to check the axis of the cylinder prescribed and also its power. It can also be used to verify that no cylindrical correction is necessary for the patient if no cylinder was detected on retinoscopy9.
The net effectof the cross-cylinder is the same as superimposing two cylindrical lenses of equal power but opposite sign with their axes at right angles. The lens is mounted on a handle which is placed at 45° to the axes of the cylinders9.
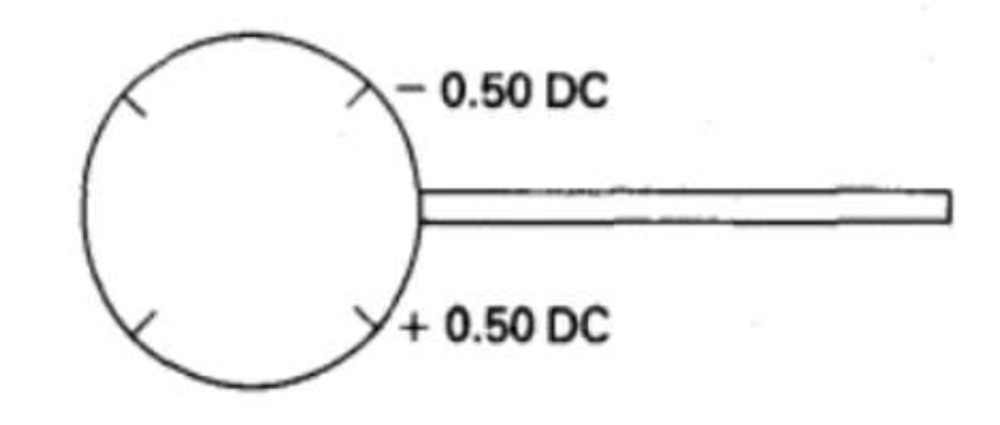
Fig. 18.A cross-cylinder -0.5 D/+1 D.
The axes marked on the lens are the axes of no power of the individual cylinders. The power of each cylinder lies at 90° to the marked axis and coincides with the marked axis of the other cylinder (of opposite sign)9.
Process of axis verification using W.D.T9:
• The cross-cylinder is held before the eye with its handle in line with the axis of the trial cylinder.
• The cross-cylinder is turned over and the patient asked which position gives a better visual result.
• The cross-cylinder is held in the preferred position and the axis of the trial cylinder rotated slightly towards the axis of the same sign on the cross-cylinder.
• The process is repeated until the trial cylinder is in the correct axis for the eye, at which time rotation of the cross-cylinder will offer equally unacceptable visual alterations to the patient.
Process of power verification using the W.D.T9:The cross-cylinder is held with first one axis and then the other overlying the trial cylinder. This has the effect of increasing and then decreasing the power of the trial cylinder.
The tumbling “E” chart was utilized for this study so as to overcome the problem ofmemorizing of optotypes by the patient.This chart is a high contrast chart containing graded letter sizes, each constructed on a grid which is 5 minutes of arc wide and 5 minutes of arc high, where the strokes on the lettersare of the size of 1 minute of arc and the width of thestroke equals the width of the gap. Each entire letter thereforesubtends an angle of 5 minutes of arc on the retina at thisdistance, but in order to analyse its form completely and seeits constituent parts, it is assumed that the eye should be ableto resolve them down to the standard limit of 1 minute of arc.
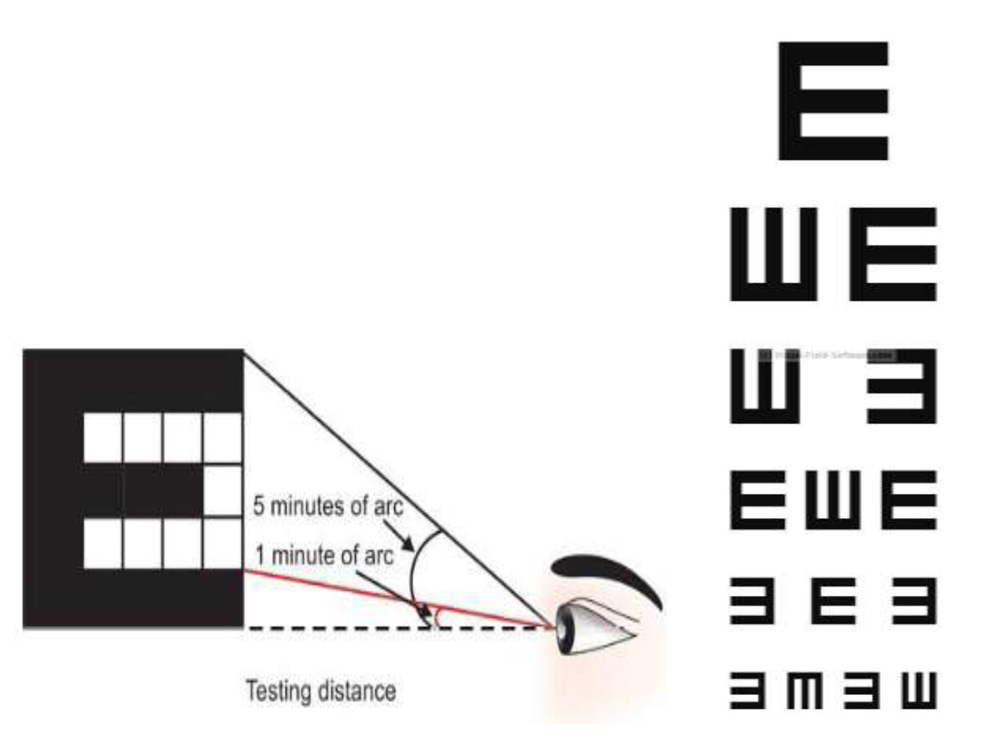 Fig. 19. The tumbling E chart(right) and its principle that each letter subtends an angle of
Fig. 19. The tumbling E chart(right) and its principle that each letter subtends an angle of
5 minutes and each stroke of a letter subtends an angle of 1minute at the nodal point(left).
OBJECTIVES
1) Correlation of static retinoscopy with monocular & binocular subjective refraction.
2) Correlation of Mohindra’s retinoscopy with monocular & binocular subjective refraction.
REVIEW OF LITERATURE
Mohindrahas found a high correlation between nearretinoscopy and subjective refraction1.
Millodot and O’Leary carried out a study on 1078 eyes of all ages and concluded that there was a hyperopic shift of 0.3-0.4 D between static retinoscopy and subjective refraction in subjects below the age of 15. The hyperopic shift diminished with age and became negative beyond the age of 50 years12.
Grosvenor et al. In their study on 100 children aged 6-10 the mean difference between static retinoscopy & subjective refraction was insignificant (0.01 D)13.
Jorge et al compared static retinoscopy with subjective refraction in 192 adults aged 18 to 34 & found an insignificant average difference of 0.02 D6.
Considering these studies the correlation between retinoscopy and subjective refraction should behigh.
Not much research has been done in this area since then. Although a few studies have used the near retinoscopy technique of Mohindra, none thus far have tried to scrutinize its relation to subjective acceptance or to static retinoscopy.
METHODOLOGY
Study design
Prospective observational study using purposive sampling.
Study sample
A sample of 100 eyes of 50 patients who came to the O.P.D of KIMS Hospital satisfying the inclusion criteria were evaluated. This is as per the recommendations of the university.
Statistical Methods
To enable a mathematical evaluation of results. The result from all the retinoscopy& refraction methods were converted into spherical equivalents using the formula:
Spherical equivalent = spherical correction + (cylindrical correction)/2
The Statistical software namely SAS 9.2, SPSS 15.0, Stata 10.1, MedCalc 9.0.1 ,Systat 12.0 and R environment ver.2.11.1 were used for the analysis of the data. Microsoft word and Excel have been used to generate graphs, tables etc.The collected data wasanalysed in Excel using two-sided paired t-test, chi square test, Pearsons correlation analysis, Bland-Altman plot, Passing &Bablok regression analysis.
Descriptive and inferential statistical analysis have been used in the present study. The results on continuous measurements have been presented on Mean SD (Min-Max) and results on categorical measurements have been presented in Number (%). Significance has been assessed at 5% level of significance.
The following assumptions on data have been made:
1.Dependent variables are normally distributed,
2.Samples were drawn from the population randomly, Cases of the samples are independent.
Inclusion criteria
- Healthy eyes with binocular vision (fusion).
- Cases with pinhole improvement in visual acuity.
Exclusion criteria
1)Non consenting patients
2)Cases with poor binocular vision including:
- tropia
- amblyopia of more than two lines difference between the eyes
The inclusion &exclusion criteria have been liberally designed with a goal to simulate the conditions & patient profilethat ophthalmologists/optometristsencounter intheir OPD’son a daily basis.
Materials
1) Heine beta 200 streak retinoscope:
The Heine beta 200streak retinoscope is the ideal instrument for this study. It is a portable, durable, handheld, battery operated instrument. The Heine Beta 200 Retinoscope with ParaStop features the latest multi-coated optics for an exceptionally bright fundus reflex and easier detection of the neutralization point.
In this study we used two 1.2V Ni-Cd rechargeable batteries. This rechargeable power source is especially useful in high patient load scenarios.
Fig. 20. Heine beta 200 streak retinoscopeand the rechargeable batteries used for this study
The unique features of this instrument include:
• The ParaStop: Precise, easy selection of a parallel beam.(fig. 8.)
• Ergonomic shape. Protects the examiner’s orbita from stray light.
• XHL Xenon Halogen Technology. Bright, white light. Bright fundus reflex, easy recognition of neutralization point.
• Metal controls. Long-lasting.
• Single control for vergence and rotation. Comfortable operation.
• Dustproof. Maintenance-free.
• Integrated polarisation filter. Eliminates stray light and internal reflexes for a brighter fundus reflex.
• Detachable brow rest. Increased comfort and control during examination especially when the operator uses glasses.
2) Tumbling “E”chart with the facility to perform the worth’s 4 dot test(W.D.T):

Fig. 21.The refraction unit where the procedures were carried out.
3) Trail frame & trial lens set (loose lenses):
Fig. 22. Trail lens set.
- The examination room – the room chosen for the study had anilluminance of 37 lux(measured with lux Meter andoid app, version 1.2, developed by Not Quite Them).
These settings were chosen so as to:
• Not be too bright – can stimulate reflex constriction of the pupil to light,
• Not be too dark – to enable the patients to have peripheral fusion which would be essential during binocular subjective vision estimation,
• The conditions also were chosen keeping in mind that they would more closely resemble a typical OPD setting.
METHODS
Static Retinoscopy:
The following steps were followed while performing static retinoscopy:
• The patient was instructed to fixate at the largest optotype of the tumbling “E” chart, 6m away. They were asked to keep the nontested eye occluded with their palm.
• The working distance was 50cm (far enough to reduce bright light induced decrease in visual acuity & close enough to enable good observation of retinoscopy reflexes).
• Retinoscopy was performed by sweeping the retinoscope beam across the vertical, horizontal & oblique meridians of the patient’s pupil & reflexes neutralized.
• All the reflexes were neutralized. The magnitude of the neutralizing lens was recorded.
• The dioptric working distance of 2.0 D is subtracted from the neutralizing lens to obtain the refractive error of the eye.
Mohindra’s near retinoscopy
The non-accommodative stimulus of the retinoscope light2 is the fixation target.Retinoscopy was performed with the non-tested eye occluded to prevent any stimuli to accommodation.
The following steps were followed while performing Mohindra’s retinoscopy:
• The patient was asked to fixate at the light of the retinoscope, using his palm to cover the untested eye.
• The working distance was 50 cm.
• Retinoscopy was performed by sweeping the retinoscope beam across the vertical, horizontal & oblique meridians of the patient’s pupil & reflexes neutralized.
• All the reflexes were neutralized. The magnitude of the neutralizing lens was recorded.
• A correction factor of 1.25 D(the dioptric working distance of -2.00D with a tonus adjustment of +0.75 D for dark focus) was subtracted from the result to obtain the refractive error of the eye.
Monocular subjective refraction.
The following steps were followed while performing monocular subjective refraction:
• The refractive error obtained during retinoscopy (static &Mohindra techniques) was the starting point.
• The non-tested eye was occluded.
• An approximate amount of spherical correction was then given to the patient to enable determination of the cylindrical elements.
• The cylinder axis was determined, followed by cylinder power.
• Then the final spherical power was refined.
Binocular subjective refraction.
The following steps were followed while performing binocular subjective refraction:
• The result of the refraction obtained during M.S.R was used as the starting point.
• Both eyes were fogged till visual acuity of 6/12 or two tumbling “E” chart lines above the unaided visual acuity was reached & fusion was maintained through the peripheral vision.
• The non-tested eye remained fogged throughout the procedure, while the tested eye was refracted following the same principles as described for monocular refraction.
• The Worth Four Dot test was used to ensure binocular vision(fusion) throughout the procedure.
RESULTS
All selected participants improved to 6/6 visual acuity onthe tumbling “E” chart on subjective refraction. The cyclindrical axes estimated by retinoscopy methods& that accepted by patients remained the same.
The mean age of patients in the study group was 29.46yrs.
60% of eyes included were of female patients & 40% were from male patients.
50% of the study sample were between the ages of 21 – 30 years, of this 56.7% of eyes belonged to female patients.
1) Static retinoscopy: The results of static retinoscopy show that the refractive errors of the patients ranged from –7.625D to +3.25D. The majority of eyes had a refractive error between -3.00D to 0(zero)D, comprising 66%. The mean spherical equivalent was -1.296D & standard deviation was 1.957.
2) Mohindra’s retinoscopy: The results of Mohindra’s retinoscopy show that the refractive errors of the patients ranged from-8.00D to +3.00D. The majority of eyes had refractive errors ranging from -2D to 0D, comprising of nearly 56%. The mean spherical equivalent was -1.154D & standard deviation was 1.853.
3) Monocular subjective refraction:The results of monocular subjective refraction show that the refractive errors of the patients ranged readings ranged from -7.625D to +3.00D. The majority of patients had refractive errors ranging from -2D to 0D, comprising 58% of eyes. The mean spherical equivalent was -1.22D & standard deviation was 1.929.
4) Binocular subjective refraction:The results of binocular subjective refraction show that the refractive errors of the patients ranged from -7D to +2.5D. The majority of patients had refractive errors between -2.00D to 0(zero)D, comprising 61%. Mean spherical equivalent was -1.029D & standard deviation was 1.774.
The Pearson’s correlation between static vsMohindra’sretinoscopy showed an “r” value of 0.954 and “p” value of <0.01.
The Pearson’s correlation between monocular vs binocular subjective refraction showed an “r” value of 0.921 and “p” value of <0.01.
The Pearson’s correlation of static retinoscopyvs monocular refraction showed an “r” value of 0.968 and a “p” value of<0.01.
The Pearson’s correlation of static retinoscopyvs binocular refraction showed an “r” value of 0.927 and a “p” value of <0.01.
The Pearson’s correlation of Mohindra’sretinoscopyvs monocular refraction showed an “r” value of 0.933 and a “p” value of <0.01.
The Pearson’s correlation of Mohindra’sretinoscopyvs binocular refraction showed an “r” value of 0.951 and a “p” value of<0.01.
The Bland-Altman plot for correlation of static vsMohindra’sretinoscopy shows a bias estimate of -0.14 with underestimate of 2 values and over-estimate of 1 value.
The Bland-Altman plot for correlation of monocular vs monocular refraction shows a bias estimate of -0.19 with underestimate of 2 values and no overestimate.
The results of Passing and Bablok regression analysis shows a plot with very good agreement between S.R & M.R and between B.S.R & M.S.R values & also the plot between these variables respectively show all values lie within allowable bias bands.
| Age in years | No. of patients | % |
| 10-20 | 14 | 14.0 |
| 21-30 | 50 | 50.0 |
| 31-40 | 22 | 22.0 |
| 41-50 | 12 | 12.0 |
| >50 | 2 | 2.0 |
| Total | 100 | 100.0 |
Mean ± SD: 29.46±10.12
Table. 4. Age distribution of patients studied
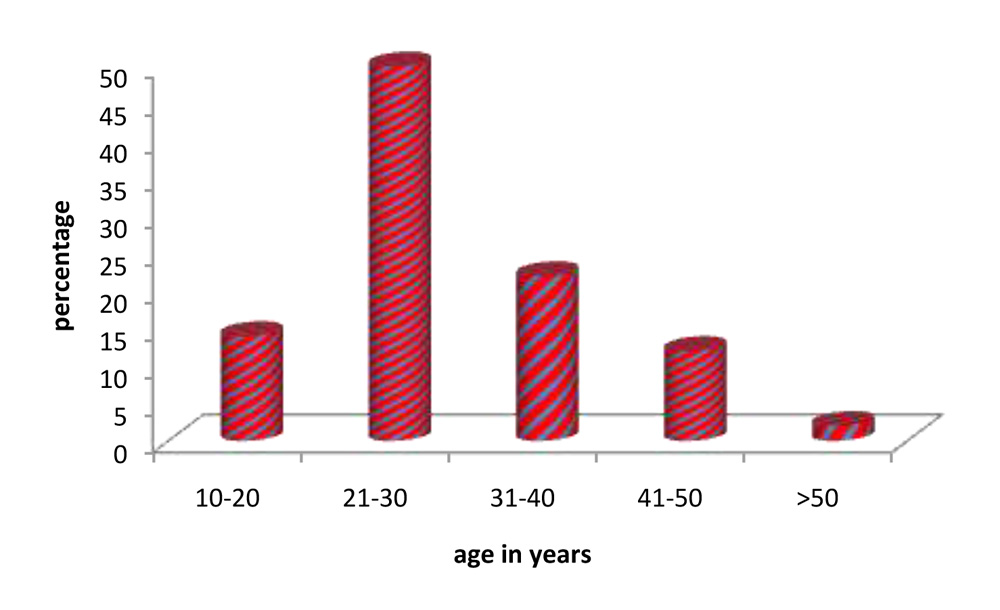
Fig. 23. Age distribution of patients studied.
The mean age of patients in the study group was 29.46yrs, a majority of the participants were females between the ages of 21-30yrs
| Gender | No. of eyes | % |
| Female | 60 | 60.0 |
| Male | 40 | 40.0 |
| Total | 100 | 100.0 |
Table 5: Gender distribution of patients studied
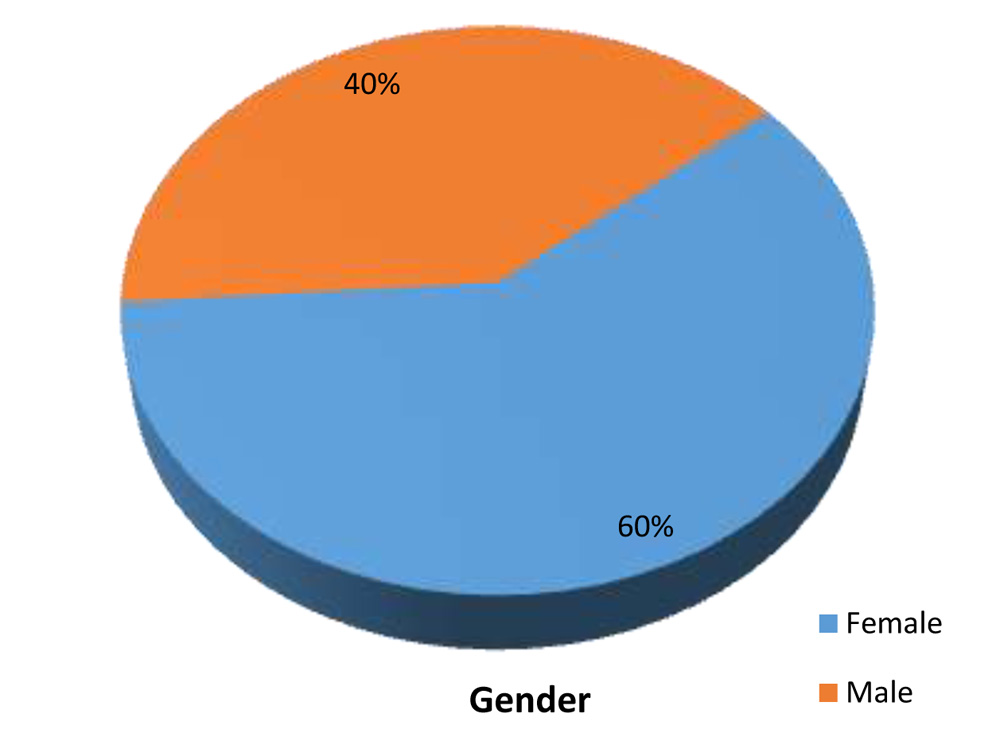
Fig. 24.Gender distribution of patients studied.
60% of eyes included were of female patients & 40% were from male patients.
| Age in years | Gender | Total | |
| Female | Male | ||
| 10-20 | 2(3.3%) | 12(30%) | 14(14%) |
| 21-30 | 34(56.7%) | 16(40%) | 50(50%) |
| 31-40 | 16(26.7%) | 6(15%) | 22(22%) |
| 41-50 | 6(10%) | 6(15%) | 12(12%) |
| >50 | 2(3.3%) | 0(0%) | 2(2%) |
| Total | 60(100%) | 40(100%) | 100(100%) |
P=0.002**, Significant, Chi-Square test
Table 6. Age & gender distribution of patients studied.
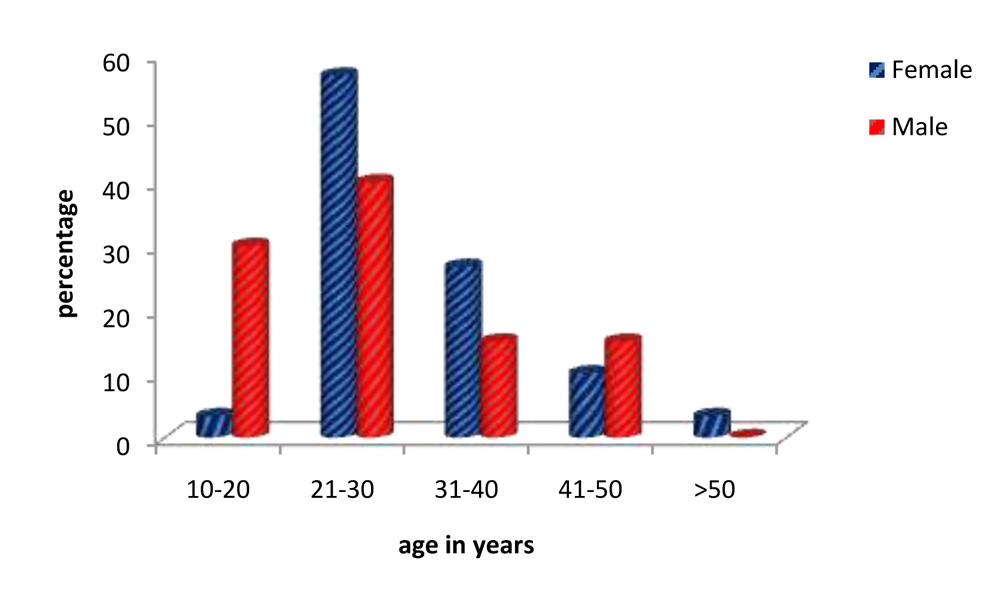
Fig. 25.Age & gender distribution of patients studied.
50% of the study sample were between the ages of 21 – 30 years, of this 56.7% of eyes belonged to femalepatients.
| Staticretinoscopy | Gender | Total | |
| Female | Male | ||
| <-3 | 10(16.7%) | 6(15%) | 16(16%) |
| -3 to 0 | 38(63.3%) | 28(70%) | 66(66%) |
| 0-3 | 11(18.3%) | 6(15%) | 17(17%) |
| >3 | 1(1.7%) | 0(0%) | 1(1%) |
| Total | 60(100%) | 40(100%) | 100(100%) |
P=0.795, Not significant, Chi-Square test
Table 7. Static retinoscopy: patient’s gender & magnitude of refractive error
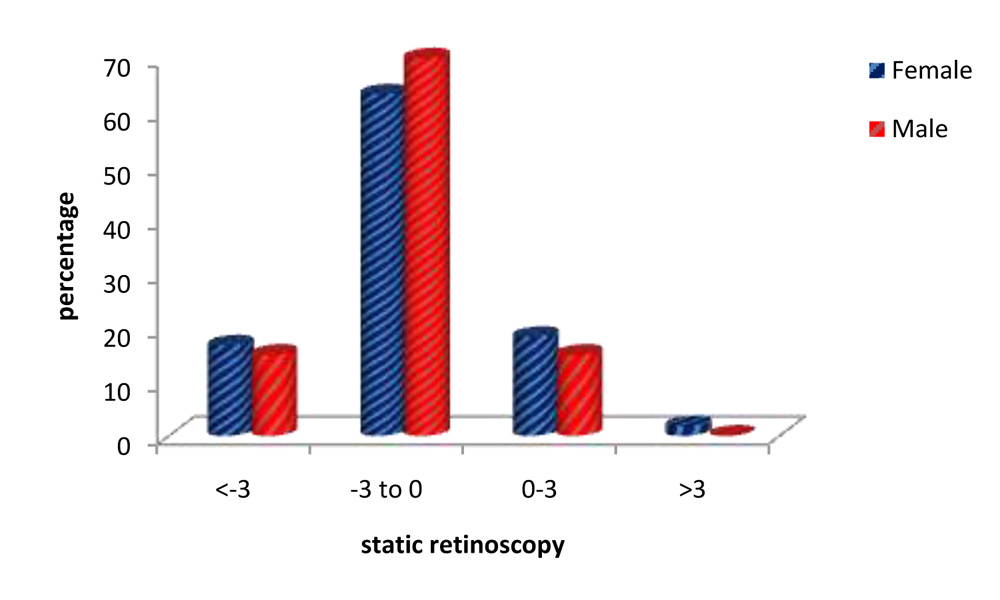
Fig. 26. Static retinoscopy: patient’s gender & magnitude of refractive error.
The results of static retinoscopy show that 66% of eyes had a refractive error between -3.00D to 0(zero)D.
| Mohindra’sretinoscopy | Gender | Total | |
| Female | Male | ||
| <-2 | 11(18.3%) | 13(32.5%) | 24(24%) |
| -2 to 0 | 37(61.7%) | 19(47.5%) | 56(56%) |
| 0-2 | 10(16.7%) | 6(15%) | 16(16%) |
| >2 | 2(3.3%) | 2(5%) | 4(4%) |
| Total | 60(100%) | 40(100%) | 100(100%) |
P=0.380, Not significant, Chi-Square test
Table 8.Mohindra’sretinoscopy: patient’s gender & magnitude of refractive error
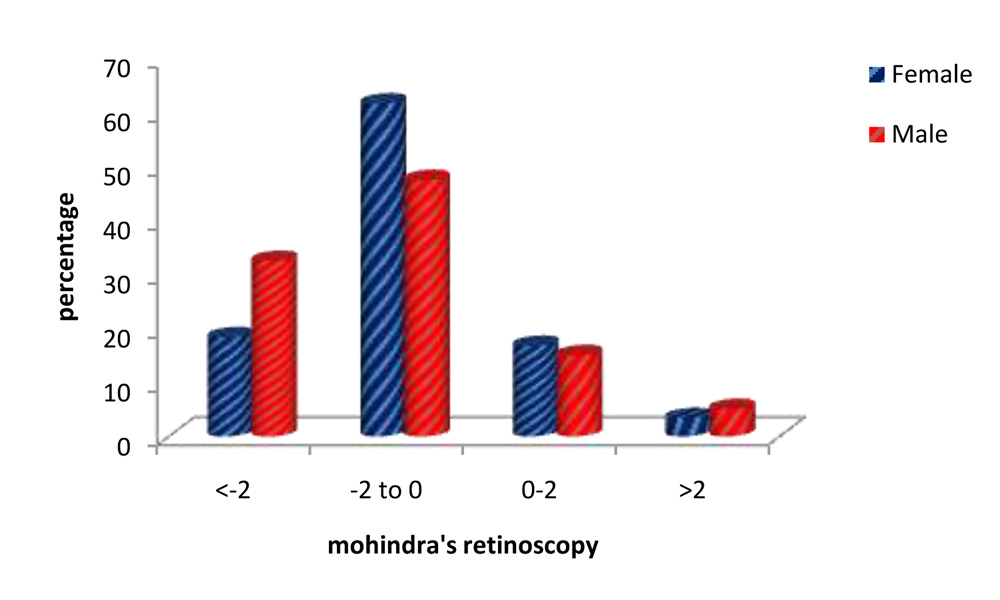
Fig. 27:Mohindra’sretinoscopy: patient’s gender & magnitude of refractive error.
The values of Mohindra’s retinoscopy show the majority of eyes had refractive errors ranging from -2D to 0D, comprising of nearly 56%.
| Monocular Subjective refraction | Gender | Total | |
| Female | Male | ||
| <-2 | 12(20%) | 13(32.5%) | 25(25%) |
| -2 to 0 | 38(63.3%) | 20(50%) | 58(58%) |
| 0-2 | 8(13.3%) | 5(12.5%) | 13(13%) |
| >2 | 2(3.3%) | 2(5%) | 4(4%) |
| Total | 60(100%) | 40(100%) | 100(100%) |
P=0.491, Not significant, Chi-Square test
Table. 9.MonocularSubjective refraction: patient’s gender & magnitude of refractive error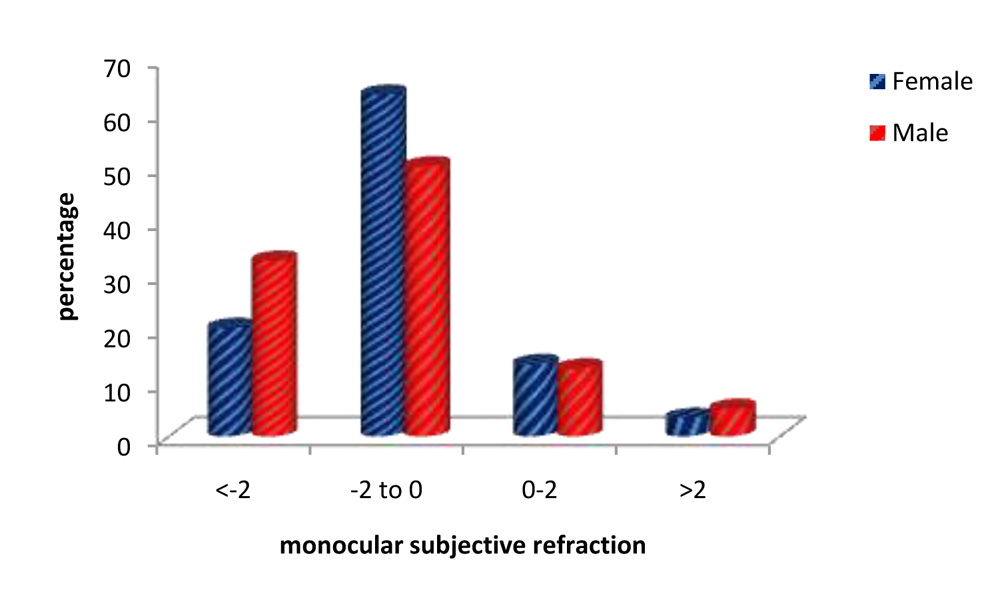
Fig. 28:Monocular Subjective refraction: patient’s gender & magnitude of refractive error.
Monocular subjective refraction readings show the majority of eyes had refractive errors ranging from -2D to 0D, comprising 58% of eyes.
| Binocular Subjective refractions | Gender | Total | |
| Female | Male | ||
| <-2 | 10(16.7%) | 10(25%) | 20(20%) |
| -2 to 0 | 40(66.7%) | 21(52.5%) | 61(61%) |
| 0-2 | 8(13.3%) | 8(20%) | 16(16%) |
| >2 | 2(3.3%) | 1(2.5%) | 3(3%) |
| Total | 60(100%) | 40(100%) | 100(100%) |
P=0.504, Not significant, Chi-Square test
Table 10: Binocular Subjective refractions: patient’s gender & magnitude of correction
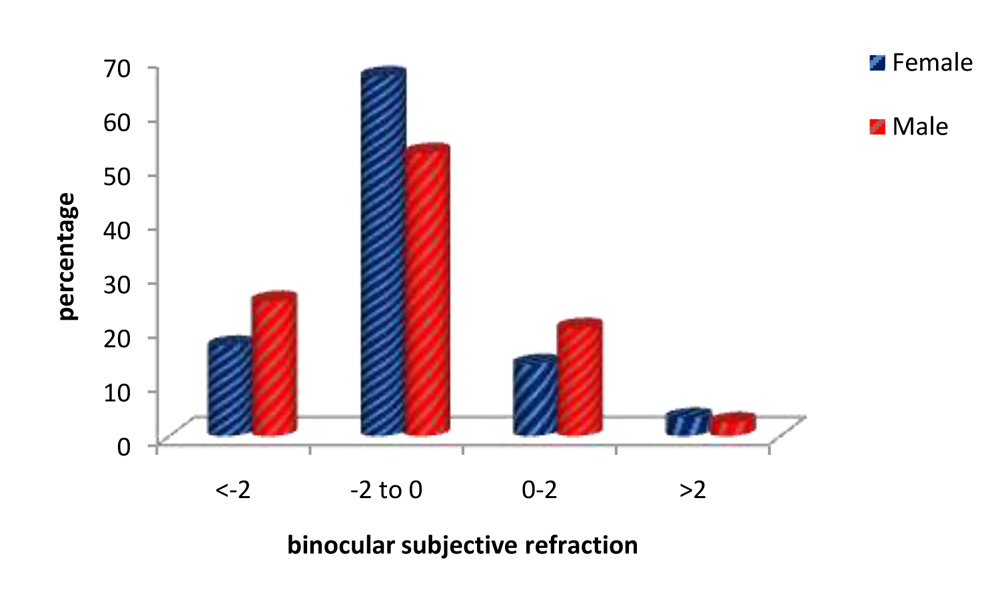
Fig. 29: BinocularSubjective refraction:patient’s gender & magnitude of refractive error
The results of binocular refraction show that the majority of eyes had refractive errors between -2.00D to 0(zero)D, comprising 61% of eyes.
| Pearson correlation | r value | P value |
| StaticretinoscopyvsMohindraretinoscopy | 0.954 | <0.01 |
Table 11: Pearson correlation: Static retinoscopyvsMohindraretinoscopy
Pearsons correlation between static &Mohindra’s retinoscopy shows a value of 0.954, indicating a high correlation.
| Pearson correlation | r value | P value |
| Monocular subjectiverefractionsvs binocular subjective refractions | 0.921 | <0.01 |
Table 12: Pearson’s correlation: Monocular subjective refractions vs binocular subjective refractions.
Pearson’s correlation between monocular & binocular subjective refraction showed a value of 0.921 indicating a high correlation.
| Bias estimate | Under-estimate | Over-estimate | |
| Static vsMohindra’sretinoscopy | -0.14 | 2 | 1 |
| Monocular vs Binocular refraction | -0.19 | 2 | 0 |
Table 13: Bland –Altman plot for correlation of Static vsMohindra’s near retinoscopy and Monocular vs Binocular refraction.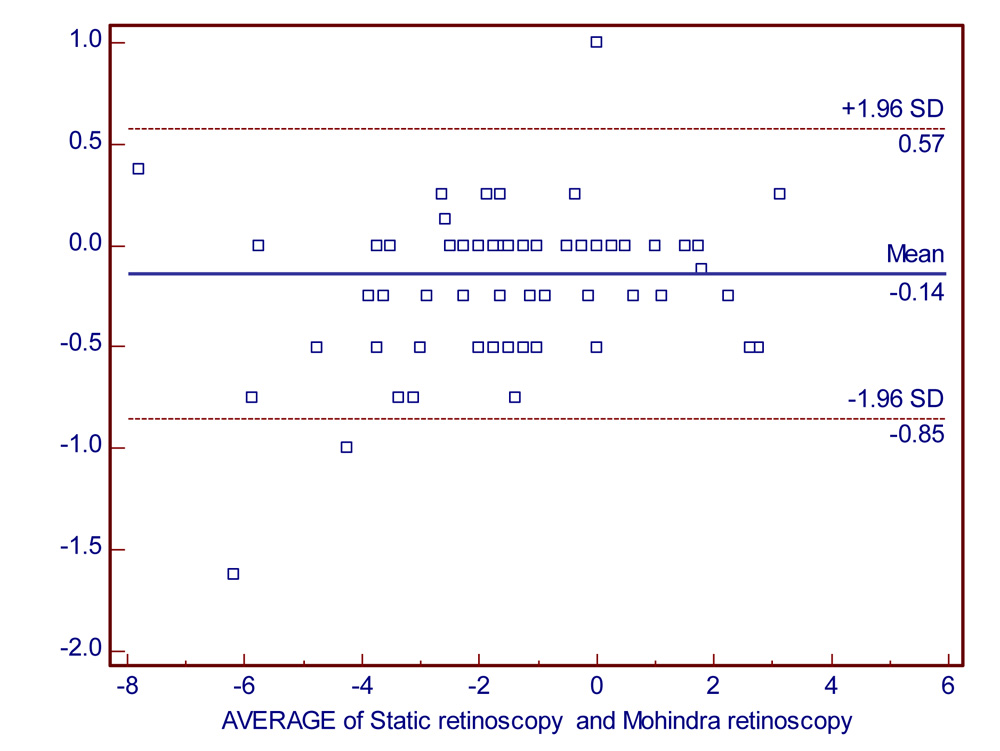
Fig 30: Bland –Altman plot for correlation of Static and Mohindra’sretinoscopy.
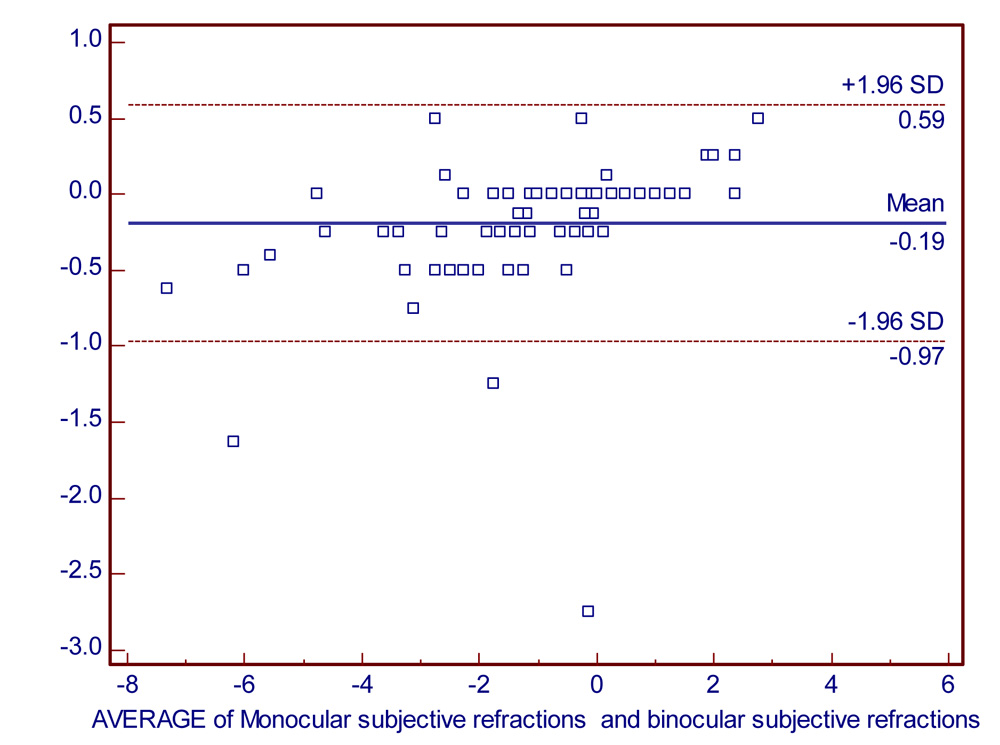
Fig 31: Bland –Altman plot for correlation of Monocular and Binocular refraction
The Bland-Altman plot of S.R vs M.R & M.S.R vs B.S.R both show a very low bias estimate & a good agreement between the values.
| Statistics | Retinoscopy | Subjective refraction | ||
| Static | Mohindra | Binocular | Monocular | |
| Lowest value | -7.625 | -8.000 | -7.000 | -7.625 |
| Highest value | 3.250 | 3.000 | 2.500 | 3.000 |
| Arithmetic mean | -1.296 | -1.154 | -1.029 | -1.220 |
| Median | -1.250 | -1.000 | -0.875 | -1.063 |
| Standard Deviation | 1.957 | 1.853 | 1.774 | 1.929 |
| Standard error of mean | 0.196 | 0.185 | 0.177 | 0.193 |
Table 14: Results on Passing and Bablok regression analysis
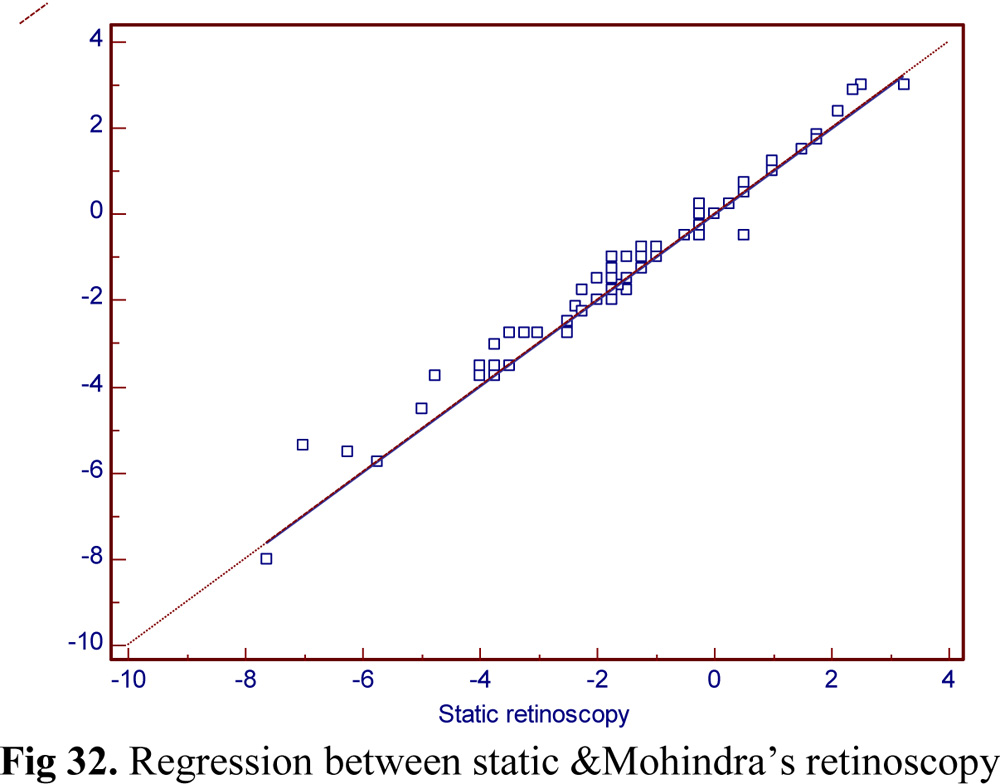
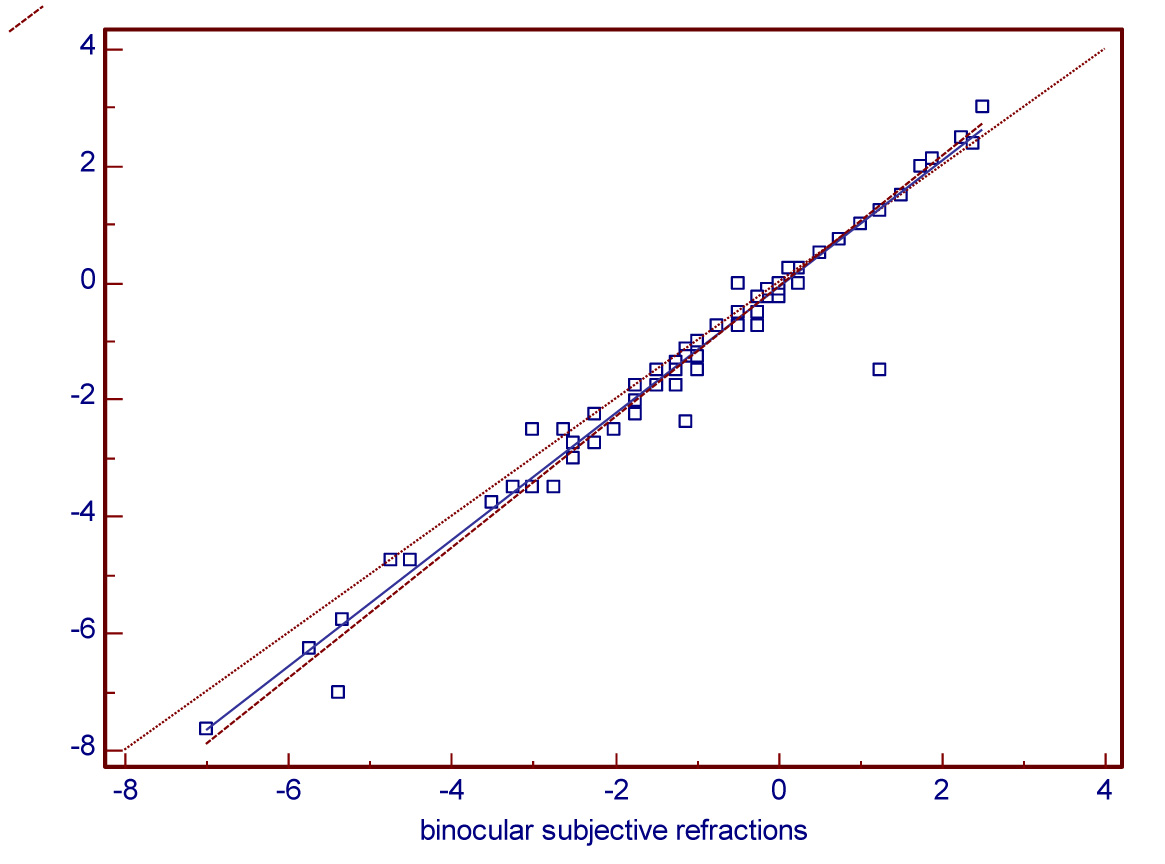
Fig 33.Regression between monocular & binocular subjective refraction.
The results of Passing and Bablok regression analysis shows a plot with very good agreement between S.R & M.R and between B.S.R & M.S.R values & also the plot between these variables respectively show all values lie within allowable bias limits.
| Pearson correlation | r value | P value |
| static retinosopyvs monocular refraction | 0.968 | <0.01** |
| static retinosopyvs binocular refraction | 0.927 | <0.01** |
| Mohindra’sretinoscopyvs monocular refraction | 0.933 | <0.01** |
| Mohindra’sretinoscopyvs binocular refraction | 0.951 | <0.01** |
Table 15: Pearson correlation comparing methods of retinoscopy with methods of refraction
M.R shows values closer to B.S.R &S.R shows values closer to M.S.R.
Significant figures
+ Suggestive significance (P value: 0.05<P<0.10)
* Moderately significant ( P value:0.01
** Strongly significant (P value: P0.01)
Statistical software: The Statistical software namely SAS 9.2, SPSS 15.0, Stata 10.1, MedCalc 9.0.1 ,Systat 12.0 and R environment ver.2.11.1 were used for the analysis of the data and Microsoft word and Excel have been used to generate graphs, tables etc.
DISCUSSION
Mohindra’s technique proved to bevery easy to perform as it was easy to get the patient to focus at the retinoscope’s light,rather than asking them to fixate at a distant optotype and ensuring good fixation.
Binocular refraction proved to be superior to monocular refraction. Here lower magnitudes of corrective lenses, compared to monocular refraction, would give the patient a better visual acuity. A majority of the patients felt happier with the result of binocular refraction.
Female patients made up the majority of the sample size, and most patients of the study sample were between the ages of 21 – 30 years.
The results showed a close correlation between all the variables considered for the study. The overall high correlation between retinoscopy and subjective refraction is a well-established fact,shown by others like Jorge et al6.
Both the methods of retinoscopy showed close correlation with each other & with the final acceptance. Pearson’s correlation between S.R & M.R and between M.S.R & B.S.R indicate a good correlation.
This shows that there is no significant difference between near retinoscopy and subjective refraction, which supports the results found by Mohindra in her paper1. Mohindra’s technique showed values closer to monocular subjective refraction than binocular subjective refraction.
There is a higher correlation between static retinoscopy and monocular subjective refraction than with binocular subjective refraction.This can be explained by the fact that the relaxation of and control over accommodation is not as good in monocular as binocular viewing.
There is a higher correlation between Mohindra’s retinoscopy and binocular subjective refraction than monocular refraction.
The Bland-Altman plot showed a very low bias estimate with the majority of the values lying with-in 2 standard deviations of the mean. This indicates good agreement between all values.
The results of Passing and Bablok regression analysis shows a plot with very good agreement between S.R & M.R and between B.S.R & M.S.R values & also the plot between these variables respectively show all values lie within allowable bias bands.
CONCLUSIONS
The results show a good correlation between all variables considered for this study.Both the methods of retinoscopy showed close correlation with each other & with the final acceptance.
It has also shown that static and Mohindra’sretinoscopy are similar, and that Mohindra’s retinoscopy is highly correlated with subjective refraction.
The results of this study show that there is no significant difference between near retinoscopy and subjective refraction, which supports the results found by Mohindra in her paper1.
Mohindra’s technique showed values closer to binocular subjective refraction than monocular subjective refraction. Static retinoscopy showed values closer to monocular subjective refractionthan binocular subjective refraction.
There is a higher correlation between Mohindra’s retinoscopy and binocular subjective refraction than monocular refraction.
This is the first study which has attempted to find a correlation between these variables, using refractive errors of such magnitude.
SUMMARY
This study titled “Correlation between retinoscopy and monocular & binocular subjective refraction” was conducted at The Department of Ophthalmology, KIMS, Bangalore after obtaining clearance from the ethical committee.
This was a prospective observational study using purposive sampling. A sample of 100 eyes of the patients who came to the O.P.D of KIMS Hospital satisfying the inclusion criteria were selected.
After obtaining consent, the patients found eligible for the study with respect to inclusion &exclusion criteria were made to undergo routine evaluation protocol for refractive error. This includes ocular examination & static retinoscopy with monocular subjective refraction.In addition to this,Mohindra’sretinoscopy& binocular subjective refraction were performed on them.
The values obtained from these two techniques of retinoscopy & two techniques of subjective refraction were converted to spherical equivalents & subjected to correlation analyses.
The results show a good correlation between all variables considered for this study.It has shown that static and Mohindra’sretinoscopy are similar.
The results of this study have shown that static retinoscopy is highly correlated with both methods of subjective refraction and has a higher correlation withmonocular than binocular subjective refraction. Mohindra’s retinoscopy is alsohighly correlated with both methods of subjective refraction and has a higher correlation with binocular subjective refraction than monocular subjective refraction.
This is the first study which has attempted to find a correlation between these variables, using refractive errors of such magnitude.
The study methodology has been optimised in every way possible to simulate a typical eye-camp scenario and to obtain mesurements that are as precise as possible, a few unique features of mention in our study are:
• The very first study to evaluate the effectiveness of Mohindra’s technique in an eye camp scenario.
• Retinoscopy done at 50cm working distance. Close enough to visualize the reflexes, distant enough to limit bright light induced decrease of visual acuity.
• Tumbling “E” chart employed to prevent memorizing the optotypes, and for illiterate patients.
• Liberally set inclusion and exclusion criteria to more closely simulate the conditions encountered routinely by ophthalmologists and optometrists.
• Avoiding cycloplegia and all its related disadvantages.
• Easier to concentrate on the retinoscope’s light than on distance optotypes.
• Patient is getting the benefit of being refracted by a binocular subjective refraction, a superior technique.
Bibliography
- Mohindra I. 1977. A non-cycloplegic refraction technique for infants and young children. J Am Optom Assoc. 48(4):518-523.
- Owens AD, Mohindra I and Held R. 1980. The effectiveness of a retinoscope beam as an accommodative stimulus. Invest Ophthalmol Vis Sci 19(8):942-949.
- Chaudhuri Z, Vanathi M. Postgraduate ophthalmology vol 1. New Delhi, India: Jaypee Brothers Medical Publishers; 2012. p. 42-43
- Benjamin WJ. Borish’s Clinical refraction, 2nd ed. Butterworth-Heinemann Elsevier;p. 682 – 762.
- Elliott DB. Clinical procedures in primary eye care, 2nd ed. Butterworth-Heinemann Elsevier. 2003. p. 97-132
- Jorge J, Quieros A, Almeida JB and Parafita MA. 2004. Retinoscopy/Autorefraction: which is the best starting point for a noncycloplegic refraction? Optom Vis Sci 83(1):64-68.
- John P. Lowery, Amy Joachim, Ronda Olson, Jessica Peel, Nicole N. Pearce autorefractionvsretinoscopy:A comparison of non-cycloplegic measures inapediatric sample Journal of Behavioral Optometry, Volume 16/2005/Number 1/Page 3
- Weinstock S, Wirtschafter J, Thomas C. A Decision-Oriented Manual of Retinoscopy. Optometry and Vision Science. 1977;54(1):64.
- Elkington A, Frank H, Greaney M, Elkington A. Clinical optics. Oxford: Blackwell Science; 1999.
- BCSC, section 3, clinical optics, American Academy of Ophthalmology, 2014. p. 93-149.
- Uveitis made simple, AIOS, CME SERIES no.20, S.R.Rathinam, All India Ophthalmological Society, 2010. p. 34-35.
- Millodot M and O’Leary D. 1978. The discrepancy between retinoscopy and subjective measurements: Effect of Age. Am J OptomPhysiol Opt. 55(5):309-316.
- Grosvenor T, Perrigin DM and Perrigin J. 1985. Three-way comparison of retinoscopy, subjective and Dioptron Nova refractive findings. Am J OptomPhysiol Opt. 62(1):63-65.