Dr. Rohan
Agashe, Dr. Prajna N V, Dr. Prajna Lalitha, Dr.Naveen Radhakrishnan
Dr. Rohan Agashe, Dr. N.V Prajna, Dr. Lalitha Prajna, Dr. Naveen Radhakrishnan
Abstract
Aim: To study the clinical profile, ocular morbidity and treatment outcomes of patients with Microsporidial Keratoconjunctivitis (MSK)
Methodology: A retrospective analysis of medical records of 550 cases with microbiologically proven MSK presenting between 2013 and 2015 was done. All patients were treated with topical fluconazole 0.3%
Results: Incidence of MSK increased 2.4 fold in the study period compared to previous three years. 95% patients had unilateral disease. Mean age of patients was 36 years. No risk factors were seen in 78% patients. Of patients who resolved, 76% patients had complete resolution by 3 weeks. Visual Acuity improved or remained same in 96% patients.
Conclusion: MSK is common in South India, occurs in healthy individuals and can be diagnosed easily by Gram stain. Visual outcomes after treatment are good. Topical fluconazole is effective in treatment. A significant proportion of these patients require treatment even after 3 weeks, having economic ramifications.
Introduction
Microsporidia are a diverse group of obligate spore forming intracellular eukaryotes that are closely related to fungi, causing keratoconjunctivitis and stromal keratitis1. The awareness of keratoconjunctivitis caused by microsporidia is increasing and more cases are being reported in the last decade.2 Initially thought to be a disease of the immunocompromised, recent large volume case series have reported microsporidial keratoconjunctivivits in healthy individuals3. Previous reports also show a seasonal trend with the majority of keratoconjunctivitis occurring in the month of August3.
Several observational case reports have studied the effects of drugs like topical Voriconazole, Itraconazole, Polyhexamethylene biguanide, Fumigalin, oral Albendazole, and procedures like repeated corneal swabbing for the treatment of microsporidial keratoconjunctivitis4-7Microsporidial keratoconjunctivitis, though more prevalent, is often misdiagnosed as adenoviral keratoconjunctivitis and is under-reported due to the lack of literature3. The aim of our study was to analyze the demographic profile, clinical features, treatment outcome and ocular morbidity of smear proven microsporidial keratoconjunctivitis in South India.
Material and Methods
The retrospective retrieval of patient data was performed after obtaining the permission of the Institutional Review board of Aravind Eye Hospital. The records of patients with clinical features of keratoconjunctivitis who presented to Aravind Eye Hospital, Madurai between January 2013 and December 2015 and who were positive on Grams smear for Microsporidiosis were reviewed to assess the demographic data, predisposing factors, clinical course, treatment and visual outcomes.
All the patients with keratoconjunctivitis underwent a comprehensive slit lamp examination by a cornea specialist. After documenting the clinical characteristics, all eyes with typical clinical features of microsporidial keratoconjunctivitis such as coarse superficial punctate epithelial keratitis were subjected to corneal scraping for Gram stain. After instilling 0.5% proparacaine in the eye, corneal scrapings were obtained using sterile cotton tipped swab and the material was smeared on a glass slide and subjected to Gram stain. Patients who had positive report for micros[poridia on smear evaluation were treated with topical 0.3% fluconazole eye drops 6 times a day.
Statistical analysis was done using statistical software STATA 11.0, USA. Continuous variable were expressed as mean (SD) and categorical variable were expressed as frequency (percentage).
Results
Five hundred and seventy seven eyes of 550 patients were involved in this study with bilateral involvement in 27(4.9%) patients. The age of the patients ranged from 6-85years (mean ± SD: 36.14 ± 15.79) with a slight male preponderance (305, 55.5%). The temporal distribution of prevalence in shown in figure 1 with a peak in the month of November (71, 12.9%) (statistical significance). 268(48.7%) patients were from Madurai district, with the rest being from the surrounding districts. There was a 2.4 fold rise in the incidence of MSK in the study period compared to previous three years.
The mean time to presentation from the onset of symptom was 6.5 days (1-30 days). Most patients did not have any history of risk factor (428; 77.8%). A history of dust falling into the eye was present in 70 (12.7%) patients, history of insect fall in 13(2.4%), exposure to contaminated water in 9 (1.6%) patients, and other factors such as trauma, oil entry, pesticide entry, body spray entry was noted in 30 (5.5%) patients.
Of the 550 patients, 166 (28.8%) did not receive any prior treatment. 285 (49.4%) patients had prior treatment with antibiotics, the most common being Chloramphenicol (25.4%), 69(12%) patients had received topical steroids, 43(7.5%) received antiviral medications, and 71(12.3%) patients received treatment with lubricants. Presenting symptoms included redness, irritation, watering, pain, lid swelling, foreign body sensation, photophobia and decrease in vision. All patients presented with pearly white coarse diffuse superficial punctuate keratitis which could be removed with a corneal swab.
Of the 550 patients, 292 (53.1%) came for follow up visits, while 258(46.9%) were lost to follow up. Of the 292 patients who followed up, 165 (76) % patients had complete resolution of disease at 3 week follow up.
Figure 1. Monthly distribution of Smear proven Microsporidial Keratoconjunctivitis in South India
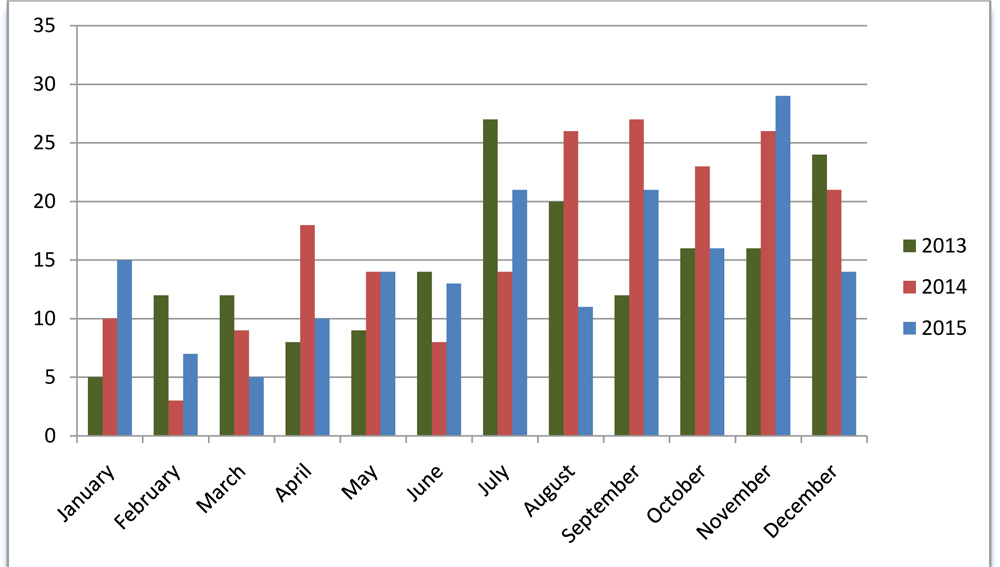
Table 1. Demographic profile of smear positive Microsporidial Keratoconjunctivitis
| Variable | n (577 eyes of 550 patients) | % |
| Gender | ||
| Male | 305 | 55.5 |
| Laterality | ||
| Bilateral | 27 | 4.9 |
| Risk factors | ||
| No risk factor | 428 | 77.8 |
| Fall of Dust | 70 | 12.7 |
| Fall of Insect | 13 | 2.4 |
| Exposure to contaminated water | 9 | 1.6 |
| Others | 30 | 5.5 |
| Previous treatment | ||
| No treatment | 166 | 28.8 |
| Antibiotic | 285 | 49.4 |
| Lubricant | 71 | 12.3 |
| Steroid | 69 | 12.0 |
| Unknown | 68 | 11.8 |
| Antiviral | 43 | 7.5 |
| Native medication | 9 | 1.6 |
Visual Acuity
The presenting visual acuity was 6/9 or better in 187 (64.0%) patients with resolved disease, while the visual acuity at resolution was 6/9 or better in 208 (70.3%) patients. Among patients who came for follow up, improvement in visual acuity was seen in 45 (15.2%) patients and no significant change was seen in 239 (80.7%). Worsening of visual acuity was noted in 12(4.1%) patients.
Discussion
Microsporidia are increasingly being recognized as a cause of keratoconjunctivitis. Prevalence of this disease has been reported from as low as 0.4% in stromal keratitis to 19.7% of all cases of keratoconjunctivitis. 8
This disease is most likely under-diagnosed and often misdiagnosed as adenoviral keratitis. A simple test such Gram staining of the epithelial samples helps in diagnosis.
The characteristic appearance is of multiple, coarse raised epithelial lesions with mild to moderate conjunctival congestion (Coarse SPKs).
Joseph et al 8 reported 19 cases of microsporidial keratoconjunctivitis in a time period of 3 years. Loh et al 7 have described 134 cases of microsporidial keratoconjunctivitis
in a span of 4 years. Das et al 9 reported 278 cases in a span of 3.5 years.
Comparatively, our study reports data of 550 patients over a period of 3 years, making it the largest single study on Microsporidial Keratoconjunctivitis (MSK) till date.
The age of the patients in our study ranged from 6 to 85 years with a mean SD: 36 +/- 16, suggesting that MSK is more common among the young adult population, compared to children and older people.
There is a male preponderance seen in our study, (55.5% vs 45.5%).
The peak prevalence was seen from July to December, not suggesting a strong correlation with rainy season, whereas earlier studies (Das et al 9) had shown peak prevalence during rainy season.
95.1% patients had unilateral disease, whereas only 4.9% had bilateral disease. However, some patients did progress from unilateral to bilateral disease.
Around 78% of our patients did not have any history of risk factors for MSK like dust entry or exposure to contaminated water, suggesting that there is no need for any specific exposure to risk factors for causing MSK.
Patients did use a variety of drugs prior to coming to our hospital. 71.2% patients had used an antibiotic (49.4%), steroid (12.0%), lubricant (12.3%) or antiviral drug (7.5%). However, there was no symptomatic relief. We did not come across any patient who was started on topical antifungal drops.
Anecdotal reports of specific drug treatment for microsporidiosis include itraconazole, albendazole, propamidine isoethionate, benzimidazole and fumagilin, but their effect remains
controversial. 4,5,6
Corneal epithelial debridement may help in debulking the load of microsporidia but according to a study by Das et al 11 it does not have any significant advantage in terms of resolution of the corneal lesions or in the final visual outcome in cases of microsporidial keratoconjunctivitis.
According to a study by Fan et al 12, repeated corneal swabbing can effectively eradicate corneal epithelial microsporidial lesions in approximately 1 week.
In our institute, we use 0.3 % topical Fluconazole eye drops in a dose of six times a day, with or without 0.3% topical ciprofloxacin eye ointment twice a day. Fluconazole is a first generation triazole antifungal.
Conclusion
Microsporidial Keratoconjunctivitis is common in South India. It occurs in healthy individuals. It is mostly unilateral and can be diagnosed easily by Gram staining. It is more common among the young adult population. Most of the patients do not have history of any risk factor. Visual outcomes after treatment are generally good. Topical Fluconazole has been effective in treating microsporidial keratoconjunctivitis. A significant proportion of patients with microsporidial keratoconjunctivitis require treatment even after 3 weeks, having significant economic ramifications.
References
- Microsporidial Keratitis: Need for Increased Awareness. Survey of Ophthalmology 2011;56(1):1–22
- Emergingprevalence of microsporidial keratitis in Singapore: epidemiology, clinical features, and management. Loh RS, Chan CM, Ti SE, Lim L, Chan KS, Tan DT. Ophthalmology. 2009 Dec;116(12):2348-53
- Clinical and Microbiological Profile of Microsporidial Keratoconjunctivitis in Southern India. Ophthalmology Volume 113, Issue 4, April 2006, Pages 531–537
- Resolution of microsporidial sinusitis and keratoconjunctivitis by itraconazole treatment. American Journal of Ophthalmology Volume 127, Issue 2, February 1999, Pages 210–212
- Clinical Trial of 0.02% Polyhexamethylene Biguanide Versus Placebo in the Treatment of Microsporidial Keratoconjunctivitis. American Journal of Ophthalmology Volume 150, Issue 1, July 2010, Pages 110–115
- Treatment of Microsporidial Keratoconjunctivitis with Topical Fumagillin. American Journal of Ophthalmology Volume 115, Issue 3, March 1993, Pages 293-298
- Treatment of Microsporidial Keratoconjunctivitis With Repeated Corneal Swabbing. American Journal of Ophthalmology Volume 154, Issue 6, December 2012, Pages 927–933
- Joseph J,Vemuganti GK, Sharma S. Microsporidia: emerging ocular pathogens. Indian J Med Microbiol. 2005 Apr;23(2):80-91
- Das S,Sharma S, Sahu SK, Nayak SS, Kar S. New microbial spectrum of epidemic keratoconjunctivitis: clinical and laboratory aspects of an outbreak. Br J Ophthalmol. 2008 Jun;92(6):861-2
- Das S,Sharma S, Sahu SK, Nayak SS, Kar S. Diagnosis, clinical features and treatment outcome of microsporidial keratoconjunctivitis. Br J Ophthalmol. 2012 Jun;96(6):793-5. doi: 10.1136/bjophthalmol-2011-301227. Epub 2012 Mar 21
- Das S,Wallang BS, Sharma S, Bhadange YV, Balne PK, Sahu SK. The efficacy of corneal debridement in the treatment of microsporidial keratoconjunctivitis: a prospective randomized clinical trial. Am J Ophthalmol. 2014 Jun;157(6):1151-5. doi: 10.1016/j.ajo.2014.02.050. Epub 2014 Feb 28
- Fan NW,Lin PY, Chen TL, Chen CP, Lee SM. Treatment of microsporidial keratoconjunctivitis with repeated corneal swabbing. Am J Ophthalmol. 2012 Dec;154(6):927-933.e1. doi: 10.1016/j.ajo.2012.06.002. Epub 2012 Sep 5