Dr. Bhushan Ghodke, G14425, Dr. Sachin Arya, Dr. ParmarGautam Singh, Dr. Ashok Kumar Meena
INTRODUCTION :
First described in 1000 BC by Susruta1,pterygium (ancient Greek “pterygon” – wing)is a triangular ‘wing-like’ growth consisting of conjunctival epithelium and hypertrophied subconjunctival connective tissue that encroaches onto the cornea. Pterygium remains an ophthalmic enigma, owing to the actual mechanism of causation. Recently,thep53 gene, a marker for neoplasia has been found in the epithelium of pterygium suggesting that pterygium may be a growth disorder due to uncontrolled cell proliferation rather than a degenerative disorder. As surgical excision is the treatment of choice, recurrence after excision isthe biggest hurdle in the success of pterygium surgery. Conjunctival autograft transplant remains the preferred treatment to prevent recurrence with high stability.2,3But the debate over the best approach has focused on whether surgeons should use sutures or sutureless options like fibrin glue to affix the conjunctival autograft.
Both methods, being popular and widely used by surgeons of Asian countries, are not perfect in the real sense of word.Pterygium surgery withfibrin glue offersadvantages such as being sutureless, shorter duration of surgery, greater patient comfort, lesser immediate postoperative pain and watering, and documented less chances of recurrences (14%) as compared to other techniques for autograft fixation.4 The disadvantages are cost and accessibility which are important factors for Indian rural population.Also, various pathogens such as parvovirus B19, human immunodeficiency virus, and Creutzfeldt-Jakob agent may be theoretically transmitted to human beings during surgery.5,6There is a report ofparvovirus B19 being clinically expressed after using fibrin glue in thoracic surgery.7Anaphylactic reactionhas also been reported after the use of (TISSEEL) fibrin sealant which was due to bovine protein aprotinin.8 In fibrin-assisted graft surgery, complications like graft dehiscence , graft retraction and pyogenic granuloma were observed more frequently.9,10
The traditional suture-assisted graft placement offers graft stability, is economical with less recurrence rates of 15%.11 The immediate patient discomfort with symptoms of pain, watering, foreign body sensation and sub-conjunctival hematoma are very common issues.12,13 Also suture removal after 2-3 weeks , especially buried knots cause great problems for the patient secondary to inflammation caused by sutures.
Thus, considering the above problems we propose a newer suture assisted technique where the autologous conjunctival graft was secured by a single 10-0 nylon suture with a releasable knot which is released on the first post-operative day and compare its results with current accepted standard of autologous blood assisted pterygium surgery.
MATERIALS AND METHODS:
It was a retrospective comparative clinical study conducted ata reputed Eye hospital inCentral India.Medical records of 197 patients with primarypterygiumwho underwent pterygium excision with conjunctivalautograftbetween January 2015 and February 2016 were reviewed. 197 eyes with different grades of pterygium were operated primarily by two techniques as decided by single author(SA).In the first group, the Releasable Suture (RS) group, the CAG was adhered to bare-sclera by a single 10-0 nylon suture tied with a releasable knot in the center of the graft-scleral bed. In the other group, the SuturelessGluefree (SG) group, patient’s own blood was used as a sealant for the CAG. All methods adhered to the tenets of the Declaration of Helsinki Principles for research on human subjects.Patients with recurrent pterygium, dry eye disease, connective tissue disorders, pseudopterygium, follow-up less than 3 months were excluded. All patients underwent routine ocular examination (visual acuity by LogMar values, refraction, laterality andanterior segment photography).
We followed the slit-lamp grading system proposedby Tan et al.14 Pterygium was graded as T1 (atrophic) – episcleral vessels underlying the body of the pterygium are unobscured,Grade T3 (fleshy) – episcleral vessels underlying the body of the pterygium aretotally obscured, and pterygia in which the episcleral vessel details were indistinctly seen or partially obscured was categorized as grade T2 (intermediate). All patients were operated by a single surgeon (SA).
Primary outcome measures were graft stability and pterygiumrecurrence. Secondary outcome measures included patient comfort in terms of pain on Visual Analogue Scale (VAS) and visual acuity.
Surgical technique :
All patients were operated under peribulbar blockunder operative ophthalmic microscope. After aseptic painting and draping, wire speculum was applied and time of commencement of surgery was noted.The body of the pterygium at limbus was held firmly by toothed forceps and adhesion between the pterygium and sclera was sharply incised and separated by using conjunctival scissors.Head of pterygium was separated from cornea and peeled off completely. The fibrous tissue was scrapped off withBard-Parker 15 number blade. After thorough dissection, the subconjunctival hypertrophied tissue was excised leaving the bare sclera exposed. Conjunctival autograft was taken from superior quadrant after inflating the conjunctiva with 0.2 cc dexamethasone injection. By careful dissection of conjunctiva with separation of underlying Tenon’s tissue, thinnest possible graft was made and incised at the limbus(conjunctivo-limbal) to involve thelimbalstem cells. Graft flip was done with 2 iris spatulas over the cornea and transferred to bare sclera area with utmost care to coincide the limbal to limbal area and epithelial side up. Ironing of the graftwith undermining the edges of CAG under the remaining host conjunctiva was done with two iris spatulas. In the RS group, centre of the graft wasfixed by a 10-0 nylon suture taken in a releasable fashion with knot kept exposed to avoid any graft disturbance during its release.In the SG group, bleeding from the surgical area was used as a source of autologous fibrin. Excessive bleeding from the site was controlled by hemostasis by sterile Merocel sponge in order to avoid graft lift by blood seepage underneath the graft.Graft was examined for apposition. Operated eye waspatched with0.3% ciprofloxacin eye ointment (Zoxan, FDC pharmaceuticals limited, India) for 24 hours.End point of surgery time was noted after removal of eye speculum. Oral ciprofloxacin 500mg tablets (Zoxan,FDC pharmaceuticals limited, India) was given twice daily for 5 days. On the first post-operative day, patient was examined on slit-lamp. Factors noted were graft apposition,adherence of autograft to scleral bed and position of knot of releasable suture in RS group. After confirmation of adequate graft apposition, the suture wasreleased on slit lamp by pulling the loose end of the 10-0 nylon suture in the RS group and patient re-examined for graft status, apposition and retraction.Patient was shown and explained the Visual Analogue Scale (VAS) with grading from 1 to 10 and asked to report the severity of pain respectively after the release of suture in RS group and in SG group respectively. Patient was asked whether he or she experienced any watering by replying in the affirmative or otherwise. Confirming favourable condition, patient was discharged on local loteprednoletabonate 0.5% ophthalmic suspension tapered over 4 weeks. Loteprednoletabonate being a ‘soft steroid’, was chosen because of its low propensity to raise intraocular pressure. All patients were followed up at 2 weeks, 3 months, 6 months and 1 year respectively.During each visit, factors studied were pain on VAS, graft apposition and recurrence. Recurrence was defined as any fibrovascularregrowth extending beyond the surgical limbus involving the cornea.
Descriptive and inferential statistical analysis was carried out in the present study. Chi-square/ Fisher Exact test wasused to find the significance of study parameters on categorical scale between the two groups.Significance was assessed at 5 % level of significance. The Statistical software namely SAS 9.2, SPSS 15.0, Stata 10.1, MedCalc9.0.1,Systat 12.0 and R environment ver.2.11.1 were used for the analysis of the data and Microsoft word and Excel have been used to generate graphs and tables.
RESULTS:
A total of 197 eyes of 197 patients underwent primary pterygium excision with conjunctival autograft secured by either of the two methods.The demographic profile of all patients is mentioned in Table 1. Both the groups were comparable in terms of demographic profile.The mean age of patient was 39.65±11.85 years and 47.36±13.84 years in RS and SG group respectively. Considering laterality, primary pterygium was present in the right eye in majority of patients included in the study. Most of the patients were of Tan’s Grade 2 primary pterygium (60% in RS group and 68% in SG group) while 40% patients were of Tan’s Grade 1 in RS group and 29% patients were of Tan’s Grade 3 in SG group. The mean surgery duration in RS group was 4.84 ±1.34 minutes with minimum of 3 minutes and maximum of 10 minutes.In SG group, the mean duration of surgery was 6.05±3.26 minutes.The pain grading on VAS from first post-operative day until 3months follow-up is shown in Table 2.In RS group, 36%patients complained of pain of scale 2 following release of suture on first post-operative day while in SG group, 44%patients had a pain scale of grade 2.Atthe 2 week follow-up visit,the pain had subsided completely in 92% of patients of RS group and in all patients of SG group. The epithelial defect was healed in all patients at second follow- up visit at 2 weeks. The preand post-operative BCVA at each visit in both the groups is shown in Table 3. In RS group, the mean BCVA before surgery was 0.27±0.41 SD which improved to 0.16±0.28 SD at 2 weeks until the last follow-up visit. In SG group, the mean pre-operative BCVA was 0.22±0.33SD which improved to 0.16± 0.22 SD during all the follow-up visits till 1 year. In both the groups, the autograft was well adhered to scleral bed at each follow-up visit with no events of complete or partial graft retraction. No intraoperative complication occurred in any patient with no serious complication post-operatively requiring any second intervention. In none of the patient, there was any sign of recurrence. All the patients strictly completed 1 year of follow-up to be eligible for inclusion in the present study.
DISCUSSION :
All the updated surgical techniques are directed to minimize the recurrence of pterygium. From the basic model of bare sclera technique to mini-Simple limbal epithelial transplant15, surgeons are in constant search for the best method that gives maximum patient comfort and least postoperative recurrence. The recurrence rate after bare sclera was highest with 88 % in certain population.16,17Kenyon et al2 and Prabhasawat et al18 demonstrated that conjunctival autograft (CAG) is the best method with lowest recurrence rate of 5.3% with highest safety margin. The main disadvantage for CAG is the use of sutures to secure the autograft to the bare sclera resulting in suture-related complications.19,20
Thus, the present retrospective comparative clinical study is intended to propose a new surgical technique which combines the gold standard technique of conjunctival autograft with the benefit of its reliable fixation with suture especially in patients coming from low socio-economic strata of developing nations and compare its results and outcomes with current standard CAG fixation method of autologous bloodassistedpterygiumsurgery
Compared to sutures, sealants like fibrin glue – popularized byKoranyi et al21 and autologous blood22,23 are more popular adjuvants to secure the CAG. But, the theoretical potential risk of transmission of infections like parvovirus-B19, hepatitis B virus, human immune-deficiency virus and anaphylaxis in susceptible individuals make fibrin glue an “off-label” adjuvant by Food and drug administration (FDA) for use in ophthalmology.22,24 Also the cost of fibrin glue equals 5 sutures thereby making it less cost-effective.21 Improper adherence of graft by fibrin glue leading to graft loss is a recognized complication.9,25,26 Lately, many studies published results of autologous blood as biological agent in pterygium surgery. But the autologous fibrin as sealant for CAG is associated with risk of graft dehiscence and graft loss requiring second surgery where another conjunctival autograft from fellow eye may be required which is ultimately affixed by sutures.27Though in our study, we did not experience any event of graft retraction (complete or partial) or graft dehiscence requiring any kind of second intervention. This may be due to use of oversized CAG with undermining of its edges beneath the host conjunctival tissue, adequate hemostasis with Merocel sponges which prevented excessive blood fromaccumulating beneath the CAG which may cause graft relift with subsequent retraction. Also, ironing of the graft with double iris spatulas yielded a better adherence of CAG with host scleral bed.
In RS group, the suture was applied in releasable fashion which helped in adherence of autograft to the scleral bed during the first 24 hours after surgery. The mean surgical time in our study was4.84±1.34 minutes. Studies in the past demonstrated thecorrelation of surgical time and success of pterygium surgery.22Increased surgical time leads to increased postoperative reaction and thus increased risk for infection.28The short time taken to apply a single releasable suture means more pterygium surgeries in less time with minimal complication rate.
Symptomatic relief of all patients in our study occurred at 2 week follow-upvisit, where patient was pain and lacrimation free which, if not better but comparable advantage in cases where fibrin glue or autologous blood is used. The pain scale on VAS was consistently less than 3in all 197 patients on first post-operative day. This result is comparable to studies where fibrin glue21 or autologous blood22,23 is used.Complications like serious inflammatoryreaction, infection, corneal ulceration, scleral melting or dellen were not noticed in any of the patient.
In our study, there were no cases with graft dehiscence or graft loss owing to the better adherence of tenon-free and large autograft to episcleral bed by suture. MitraS et al28mentioned that, once the conjunctival autograft stays in place for the first 24-48 hours, it is going to stick around. Thus the use of single suture for the first 24 hours gives a psychological relief to the surgeon ensuring better adherence and saves the patient from a second intervention following the use of sutureless adjuvants like fibrin glue and autologous blood.
The reported recurrence rate after CAG for pterygium surgery is 2% to 39%.29,30S E Tiet al11 documented that the success of pterygium surgery depends on the dissection of thinnest possible CAG (tenon-free and without buttonholing) and experience of the operating surgeon.Hirst et al31reported that there would be 97% chance of recurrence in first 12 months of pterygium surgery. In our study, there were no recurrence at any stage during the one year follow-up. This may be due to the surgical technique of thin dissection method and large CAG, secured adherence by single suture and proper edge alignment of CAG by suture and experience of the operating surgeon.
Our study hasseveral limitations. First, its retrospective study designwith no comparative group may limit its wide acceptance among ophthalmic surgeons. Secondly ,a relatively small sample size of 150 patients. Third, a follow-up of 1 year which may not be a sufficient period to comment on the efficacy of our technique in terms of recurrence.Further evaluation is required for the recurrence rate with larger sample size and randomized controlled trials are required in future.
Thus, Releasable suture mayoffer aneconomical, simple, easy to learn,fasterand a reliable method to secure the CAG resulting in least complication and nilrecurrence. The patient comfort was comparable to sutureless techniques like fibrin glue or autologous blood.
Funding/Support: No funds, grants or other support were received.
Financial Disclosures: No financial disclosures.
Other Acknowledgments: There were no conflicts of interest
REFERENCES :
- Singh G. Pterygium and its surgery. In: Foster CS, Azar DT, Dohlman CH, eds.Smolin and Thoft’sThe Cornea: scientific foundations and clinical practice. 4th edn.Vol 4. Philadelphia: Lippincott Williams & Wilkins, 2005:999–1017.
- Kenyon KR, Wagoner MD, Hettinger ME. Conjunctival autograft transplantation for advanced and recurrent pterygium. Ophthalmology 1985;92:1461–70.
- Chen PP, Ariyasu RG, Kaza V, et al. A randomized trial comparing mitomycinC and conjunctival autograft after excision of primary pterygium [see comments]. Am J Ophthalmol1995;120:151–60.
- Srinivasan S, Dollin M, McAllum P, et al. Fibrin Glue versus sutures for attaching the conjunctival autograft in pterygium Surgery: A prospective observer masked clinical trial. Br J Ophthalmol2009;93:215–8.
- Ma DH, See LC, Liau SB, Tsai RJ. Amniotic membrane graft for primary pterygium: comparison with conjunctival autograft and topical mitomycin C treatment. Br J Ophthalmol2000;84:973–8.
- Foroutan A, Beigzadeh F, Ghaempanah MJ, Eshghi P, Amirizadeh N,Sianati H, et al. Efficacy of autologous fibrin glue for primary pterygium surgery with conjunctival autograft. Iranian J Ophthalmol2011;23:39–47
- Hino M, Ishiko O, Honda KI, et al. Transmission of symptomatic parvovirus B19 infection by fibrin sealant used during surgery. Br J Haematol2000;108:194-5
- Oswald AM, Joly LM, Gury C, Disdet M, Leduc V, Kanny G. Fatal intraoperative anaphylaxis related to aprotinin after local application of fibrin glue. Anesthesiology2003;99:762–3.
- Uy HS, Reyes JM, Flores JD, Lim-Bon-Siong R. Comparison of fibrin glue and sutures for attaching conjunctival autografts after pterygium excision. Ophthalmology 2005;112:667 71.
- Srinivasan S, Slomovic AR. Eye rubbing causing conjunctival graft dehiscence following pterygium surgery with fibrin glue. Eye 2007;21:865–7.
- Ti SE, Chee SP, Dear KB, et al. Analysis of variation in success rates in conjunctival autografting for primary and recurrent pterygium. Br J Ophthalmol. 2000;84:385–389.
- Fan Xu, Min Li, Yumei Yan, Kewei Lu, Ling Cui, Qi Chen . A Novel Technique of Sutureless and Glueless Conjunctival Autografting in Pterygium Surgery by Electrocautery Pen. Cornea 2013;32:290–295
- YaseminOzdamar, SedaMutevelli, Unsal Han, Dilek_I leri, BinnurOnal, OzgurIlhan, JaleKarakaya, and OrhanZilelioglu. A Comparative Study of Tissue Glue and Vicryl Suture for Closing Limbal–Conjunctival Autografts and Histologic Evaluation After Pterygium Excision. Cornea 2008;27:552–558
- Tan DTH, Chee SP, Dear KBG, Lim ASM: Effect of pterygium morphology on pterygium recurrence in a controlled trial comparing conjunctival autografting with bare sclera excision. Arch Ophthalmol1997; 115:1235-1240.
- Hernández- Bogantes E, Amescua G, Navas A, et al. Minor ipsilateral simple limbal epithelial transplantation (mini-SLET) for pterygium treatment. Br J Ophthalmol 2015;99: 1598–1600.
- Youngson RM. Recurrence of pterygium after excision. Br JOphthalmol1972;56:120.
- Sanchez-Thorin JC, Rocha G, Yelin JB. Meta-analysis on the recurrence rates after bare sclera resection with and without MMC use and conjunctival autograft placement in surgery for primary pterygium. Br J Ophthalmol 1998;82(6):661-665
- Prabhasawat P, Barton K, Burkett G, et al. Comparison of conjunctival autografts, amniotic membrane grafts, and primary closure for pterygium excision. Ophthalmology 1997;104:974–85.
- Allan BD, Short P, Crawford GJ, Barrett GD, Constable IJ. Pterygium excision with conjunctival autografting: an effective and safe technique. Br J Ophthalmol 1993; 77: 698–701.
- Tan D. Conjunctival grafting for ocular surface disease. CurrOpinOphthalmol 1999; 10: 277–281.
- Koranyi G, Seregard S, Kopp ED. The cut-and-paste method for primary pterygium surgery: Long-term follow-up. ActaOphthalmolScand2005;83:298–301
- Kurian A, Reghunadhan I, Nair KGR. Autologous blood versus fibrin glue for conjunctival autograft adherence in sutureless pterygium surgery: a randomised controlled trial. Br J Ophthalmol2015;99:464–470
- D de Wit, I Athanasiadis, A Sharma, J Moore. Sutureless and glue-free conjunctival autograft in pterygium surgery: a case series. Eye (2010) 24, 1474–1477
- Stephen C. Kaufman, Deborah S. Jacobs, W. Barry Lee, Sophie X. Deng et al. Options and Adjuvants in Surgery for Pterygium. Ophthalmology 2013;120:201–208
- Jiang J, Yang Y, Zhang M, et al. Comparison of fibrin sealant and sutures for conjunctival autograft fixation in pterygium surgery: one-year follow-up. Ophthalmologica2008;222:105– 11.
- Karalezli A, Kucukerdonmez C, Akova YA, et al. Fibrin glue versus sutures for conjunctival autografting in pterygium surgery: a prospective comparative study. Br J Ophthalmol2008;92:1206 –10.
- Foroutan A, Beigzadeh F, Ghaempanah MJ, Eshghi P, Amirizadeh N, Sianati H, et al. Efficacy of autologous fibrin glue for primary pterygium surgery with conjunctival autograft. Iranian J Ophthalmol2011;23:39–47
- Mitra S et al. Autoblood as Tissue Adhesive for Conjunctival Autograft Fixation in Pterygium Surgery. Poster presented at the Annual Meeting of the American Academy of Ophthalmology; Oct. 22 and 23, 2011; Orlando, Fla.
- Hirst LW. The treatment of pterygium. SurvOphthalmol. 2003;48: 145–180.
- Ang LP, Chua JL, Tan DT. Current concepts and techniques in pterygium treatment. CurrOpinOphthalmol.2007;18:308–313.
- Hirst LW, Sebban A, Chant D. Pterygium recurrence time.Ophthalmology1994;101:755–8
| VARIABLES | CATEGORIES | RS GROUP | SG GROUP
|
| AGE (in years) | <20 | 1(0.7%) | 0(0%) |
| 20-30 | 42(28%) | 8(17%) | |
| 31-40 | 51(34%) | 11(23.4%) | |
| 41-50 | 36(24%) | 9(19.1%) | |
| 51-60 | 12(8%) | 11(23.4%) | |
| >60 | 8(5.3%) | 8(17%) | |
| Mean age (years) | 39.65±11.85 | 47.36±13.84 | |
| GENDER | Male | 62(41.3%) | 25(53.2%) |
| Female | 88(58.7%) | 22(46.8%) | |
| EYE INVOLVED | Left | 51(34%) | 22(46.8%) |
| Right | 99(66%) | 25(53.2%) | |
| PTERYGIUM GRADE | 1 | 60(40%) | 1(2.1%) |
| (TAN et al) | 2 | 90(60%) | 32(68.1%) |
| 3 | 0 | 14(29.8%) | |
| SURGERY DURATION
(minutes) |
1-5 | 109(72.7%) | 12(25.5%) |
| 6-10 | 41(27.3%) | 35(74.4%) | |
| Mean duration (minutes) | 4.84±1.34 | 6.05±3.26 |
TABLE 1 – PATIENT DEMOGRAPHIC PROFILE AND OTHER VARIABLES
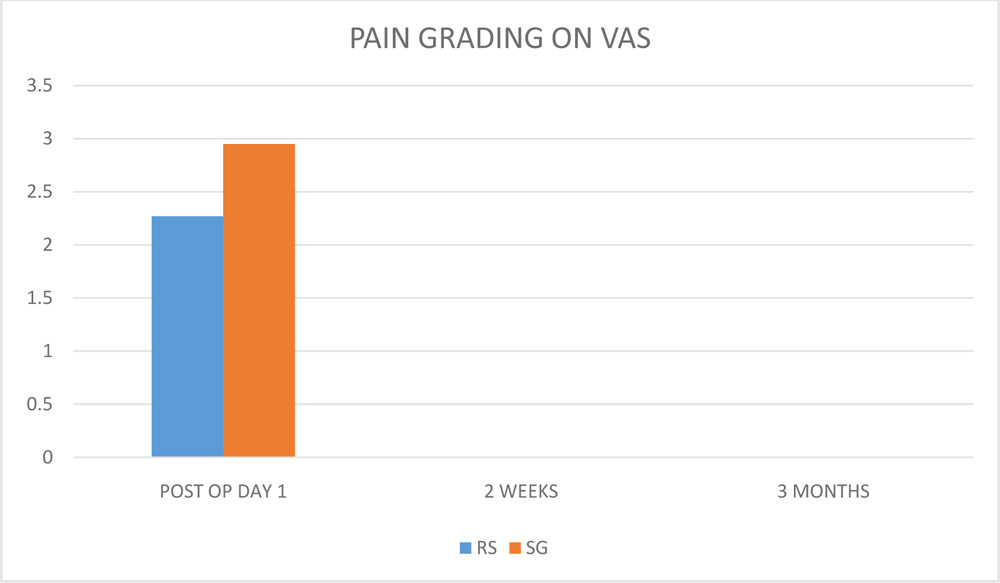
FIGURE 2 : DISTRIBUTION OF PAIN ON VISUAL ANALOQUE SCALE (VAS) IN BOTH GROUPS
( RS- RELEASABLE SUTURE GROUP, SG- SUTURELESS GLUEFREE GROUP )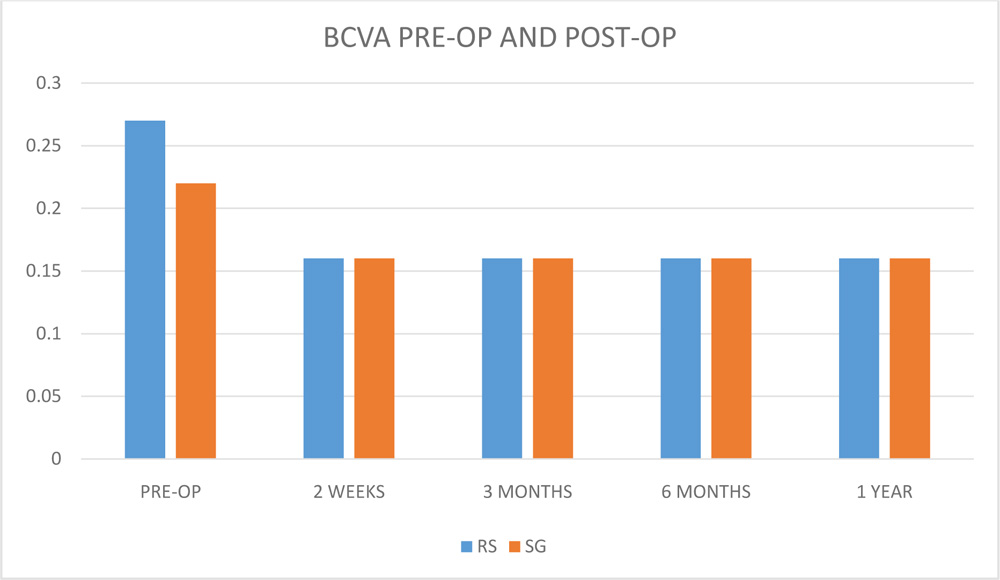
FIGURE 3: DISTRIBUTION OF BEST CORRECTED VISUAL ACUITY (BCVA) BEFORE AND AFTER PTERYGIUM SURGERY ( RS – RELEASABLE SUTURE GROUP , SG – SUTURELESS GLUEFREE GROUP )