Dr.Karishma Goyal,
S17505, Dr. Nagendra
Shekhawat, Dr. Sonal Kalia
PURPOSE- To report results of intrascleral fixation of 3-piece IOL in ciliary sulcus
METHOD- It is a prospective study of intrascleral fixation of haptic in 50 eyes by T fixation technique. Preoperative & post-operative visual acuity, Slit lamp & Fundus examination, Applanation tonometry, Keratometry, Biometry, OCT, Scheimpflug imaging done for extensive evaluation
RESULTS- There was one case in which haptic broke during handshake maneuver & another IOL was required. Postoperative complications included corneal edema (4 %), increased IOP (6 %), CME (2%), Decentration (4 %) & Dislocation (2 %), which were all managed to the level of good visual recovery. There was no significant change in corneal astigmatism. Significant change found in BCVA & UCVA after surgery
CONCLUSION- After extensive 1 year follow up with evaluation of variety of parameters, we found sutureless glueless intrascleral fixation technique, in cases with deficient posterior capsular support, safe & innovative
Introduction
Cataract surgery has become the most commonly performed intraocular procedure, with constantly improving outcomes. The intracapsular technique had been popular until the early 1980’s. Planned extracapsular cataract extraction gradually became more widespread1. It was then further refined by phacoemulsification. With the intracapsular method, there was no provision for support of an intraocular lens by lens capsule. This also happened when extracapsular methods were complicated by marked zonular dehiscence or a large posterior capsular break without an intact capsulorrhexis2. Less commonly traumatized eye, Ectopia lens or paediatric lensectomies resulted in an absence of capsular support. In aphakics visual rehabilitation can be achieved by spectacles, contact lens or intraocular lens implantation including anterior chamber IOL, iris fixated IOL or scleral fixated IOL3. Spectacles4 are associated with image magnification, roving ring scotoma, jack in box phenomenon while contact lens5 have limited use in cooperative patients & can cause dry eye, keratitis. These problems limited the use of these modalities in day to day life. Then came the concept of intraocular lens implantation6.
In the eye without an intact posterior capsule an IOL can be inserted in posterior chamber only if it is fixed with sclera. The posterior chamber is the normal anatomic position of the human lens. Thus, placement of the IOL in the posterior, rather than the anterior chamber7, 8 reduces the risk of bullous keratopathy, damage to anterior chamber angle structures, damage to corneal endothelium, pupillary block glaucoma, and pseudophakodonesis (excessive mobility of the IOL). In addition, positioning the lens closer to the rotational centre of the eye, just anterior to the vitreous face, may reduce the centrifugal forces on the lens and stabilize the ocular contents, thereby decreasing the probability of complications such as iritis, CME, and retinal detachment. Another advantage of positioning the lens closer to the nodal point and centre of rotation of the eye is the superior optical properties accrued by the lens in this position.
We evaluated a new technique of intrascleral fixation of three piece IOL without the use of suture & glue.
Material & method
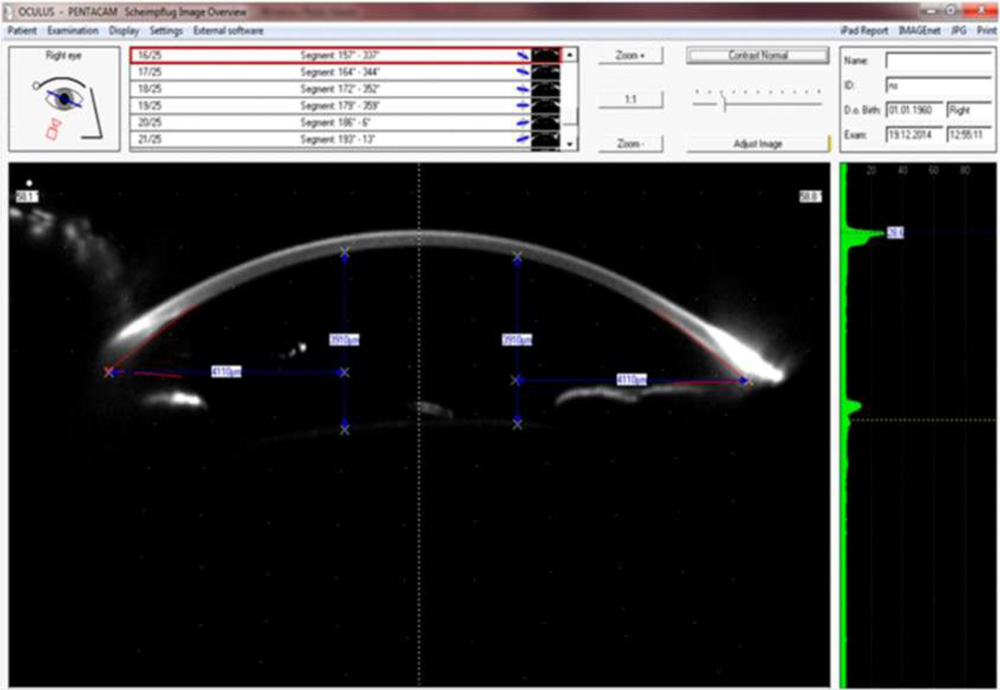
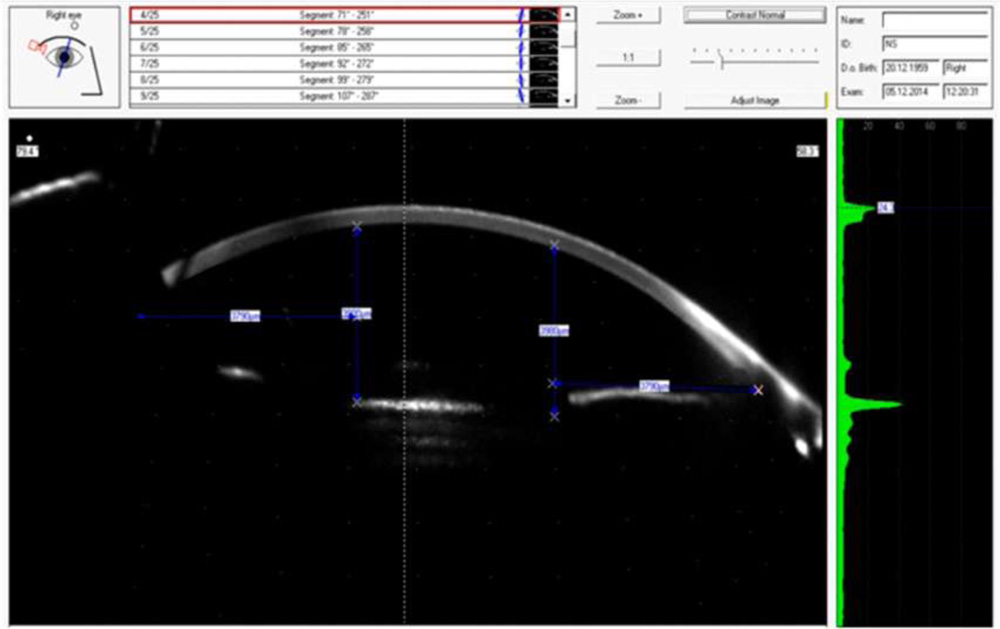
It was hospital based Descriptive type of Observational study included 50 eyes of 50 patients. Preoperative & post-operative visual acuity, Slit lamp & Fundus examination, Applanation tonometry, Keratometry, Biometry, optical coherence tomography(OCT) was done for extensive evaluation of anterior & posterior segment. Scheimpflug imaging was done to evaluate proper centration of IOL. Follow up was done on 1st, 7th, 28thpost-operative day, at month& 6 month.
Surgical technique-
Under Peribulbar anesthesia, 5.0 mm conjunctival peritomy was done at the 2 o’clock and 8 o’clock positions. Then, 2 T-shaped incisions were made 2.0mmfrom the limbus exactly 180 degrees apart diagonally. An infusion cannula or anterior chamber maintainer was inserted. To prevent interference with creation of the T-shaped incision, the infusion cannula should be positioned at 4 o’clock. Anterior vitrectomy (deep core) was performed, if necessary. Sclerotomy was done parallel to the iris at the T-shaped incision with a 23-gauge angled microvitreoretinal (MVR) knife and a scleral tunnel was made parallel to the limbus at the branching point of the T-shaped incision. 2.8 mm keratome was used to make a corneal incision at 10 o’clock through which IOL was implanted with an injector; the trailing haptic was left outside the incision. The tip of the haptic was then grasped with 24-gauge IOL haptic gripping forceps, pulled through the Sclerotomy, and externalized on the left side. After the trailing haptic was inserted into the anterior chamber& the haptic tip was grasped with a 24-gauge forceps, pulled through the second sclerotomy and externalized on the right side. The haptic insertion into the anterior chamber may be difficult depending on the material or shape of the haptics, which can cause the IOL to rotate clockwise and the leading haptic to slip back into the eye. To prevent such risks, the IOL optic was pushed to the back of the iris and moved to the 2 o’clock position with a push-and-pull hook inserted through the side port at the 1 o’clock position. The tip of the haptic was subsequently inserted into the limbus–parallel scleral tunnel. A single 8-0 vicryl suture is used to fixate the haptic to the scleral bed to prevent it from shifting immediately after surgery.
Results-
The study population consisted of 50 patients (24 female & 26 male). Mean age was 60.2 year (standard deviation 11.4 year). The minimum age was 25 year while maximum age of patient was 80 year.Table 1 shows the preexisting ocular conditions, the most common of which were aphakia during cataract surgery.
| Diagnosis | No. | % |
| Aphakia after complicated cataract surgery | 24 | 48.0% |
| Aphakia after ICCE 15 year back | 1 | 2.0% |
| Aphakia after ICCE for subluxated crystalline lens | 1 | 2.0% |
| Aphakia with cortical matter in vitreous | 1 | 2.0% |
| Dropped IOL | 4 | 8.0% |
| Nucleus drop | 5 | 10.0% |
| Operated limboscleral tear repair + subluxated traumatic cat | 1 | 2.0% |
| Subluxated cataractous lens | 4 | 8.0% |
| Subluxated IOL | 1 | 2.0% |
| Subluxated traumatic cataract with IOFB | 1 | 2.0% |
| Traumatic cataract with IOFB | 2 | 4.0% |
| Traumatic posterior dislocated crystalline lens | 3 | 6.0% |
| Traumatic posterior dislocated IOL | 1 | 2.0% |
| Traumatic subluxated IOL with inferior retinal dialysis | 1 | 2.0% |
| Grand total | 50 | 100% |
Table 1
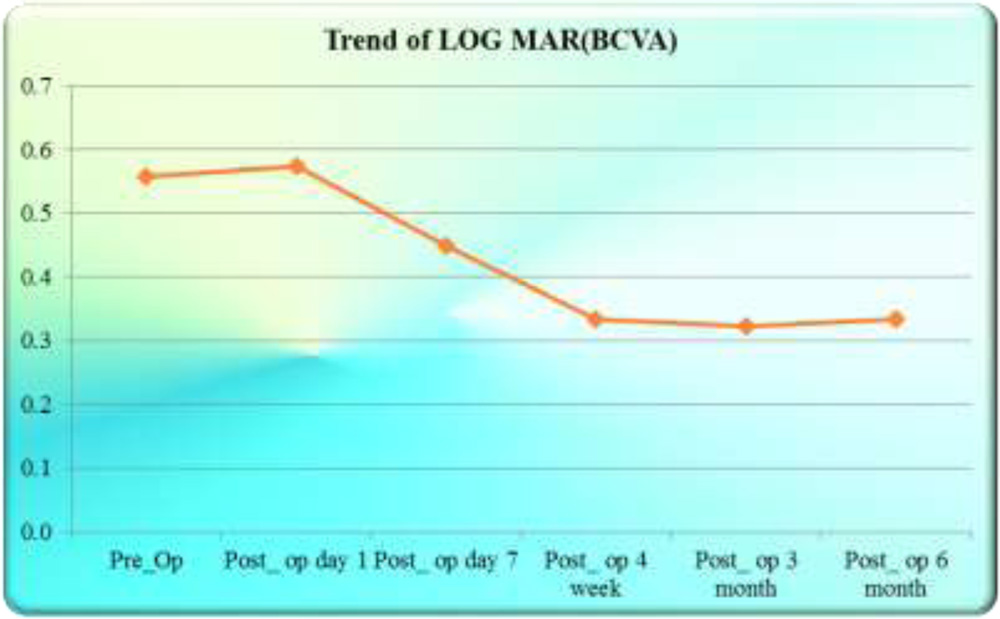
Change in uncorrected visual acuity(UCVA) in LOGMAR from pre-operative value to every follow up post operatively was highly significant (0.0000).
Changes in best corrected visual acuity (BCVA) in LOGMAR from preoperative to day 1 follow up was not significant (p=0.6842) but on next follow up change was significant (p=0.0183) and later on every follow up change was highly significant (p=0.0000).
Corneal topography & astigmatism was measured using scheimpflug imaging preoperatively & on final follow up at 6 month.Changes in K1, K2 & Astigmatism was found insignificant (0.6324, 0.4556 & 0.0510 respectively) (table 2)
| Mean | SD | p-value | |
| Pre-operative K1 | 43.2 | 2.0 | |
| Post op 6 month K1 | 43.3 | 1.8 | 0.6324 |
| Pre-operative K2 | 44.6 | 2.0 | |
| Post op 6 month K2 | 44.5 | 1.9 | 0.4556 |
| Pre-operative astigmatism | 2.0 | 1.8 | |
| Post op 6 month astigmatism | 1.8 | 1.6 | 0.0510 |
Table 2
Complications were noted on each follow up.
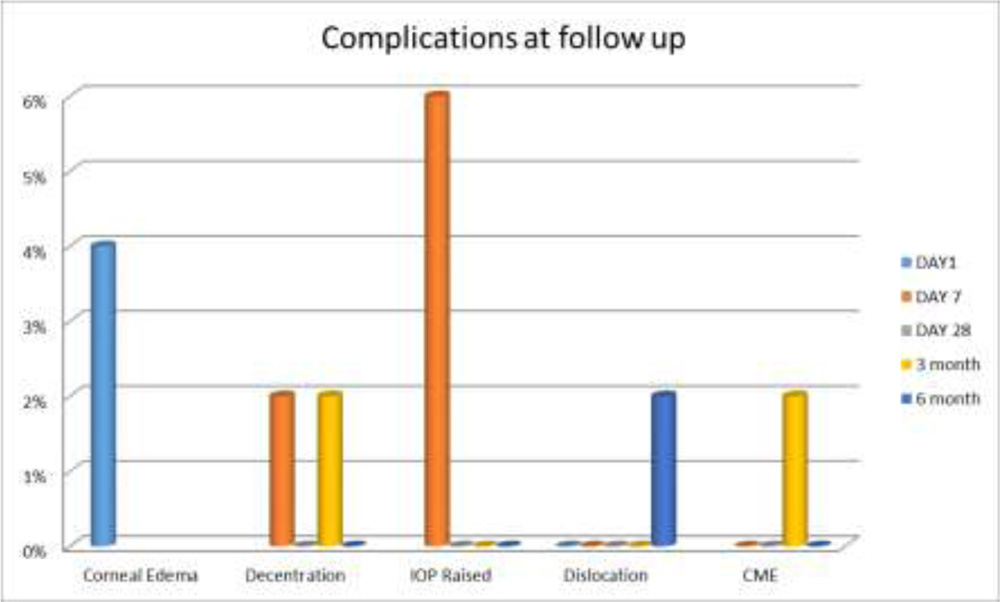
On day 1, there were 2 (4%) cases of corneal edema due to surgical manipulations which got resolved on next follow up, on day 7 there were 3(6%) cases of raised IOP which were managed medically and 1 (2%) case of decentration which was recentered surgically, at 3 month, there was 1 (2%) case of CME which was managed medically and 1 (2%) case of decentration which was recentered surgically. At the end, all have well centered IOL with good visual acuity
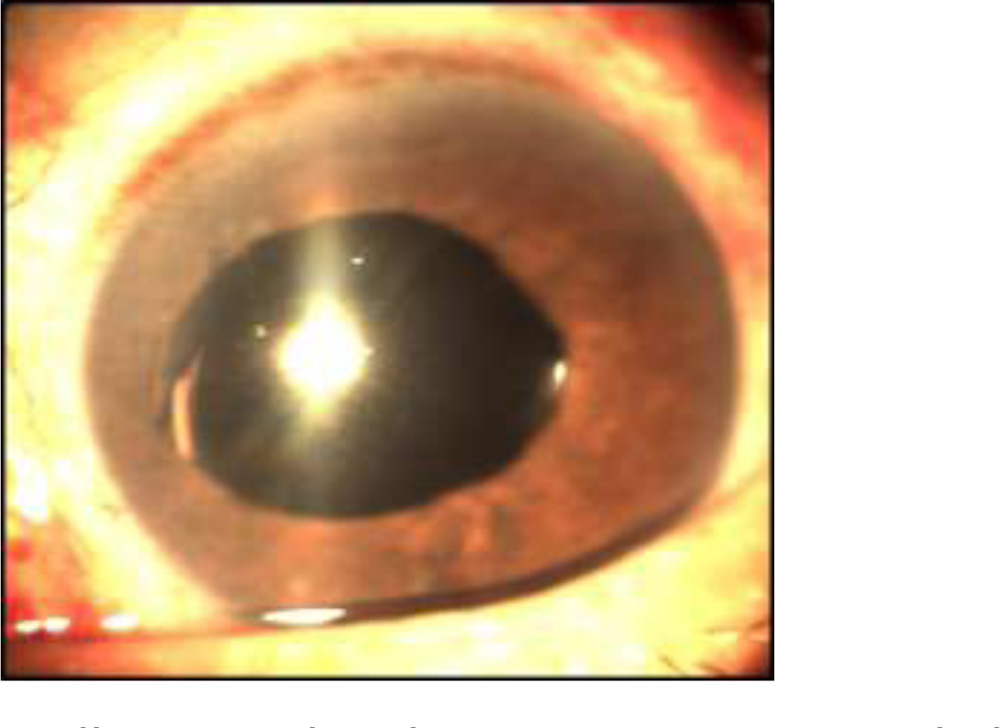
Well Centered Multipiece IOL as seen on slit lamp.
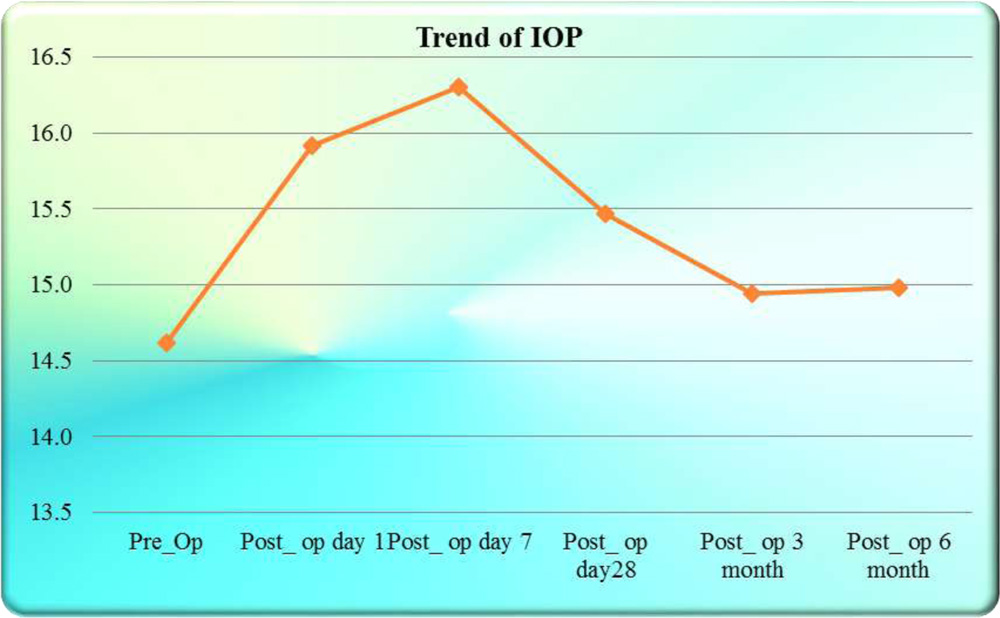
Mean IOP was 14.6±3.2 mmHg preoperatively while it was 15.00±1.7 mmHg postoperatively at 6 month. Mean IOP change from preoperative period to 6 weeks postoperative period was not statistically significant p=0.4980. • Mean change in IOP from preoperative period to post op day 1 (p=0.0110) and post op day 7(p=0.0300) was found significant as there were some case of raised IOP due to inflammation or pigment release due to maneuvering. These cases were treated medically and on next follow up their IOP came out normal.
Discussion-
The endocapsular placement of an intraocular lens (IOL) is undoubtedly anatomically most preferable following successful cataract extraction as implantation of an IOL in the capsular bag provides stable fixation at a position closest to the nodal point of the eye. Intraocular lens implantation (IOL) in the eyes that lack posterior capsular support is a problem for cataract surgeons for a long time. It is not only due to the visual outcome but also to the related complications they face in the post-operative period. In eyes with insufficient orno capsular support, IOL implantation and fixation techniques are still controversial. Many reports in the literature confirm that anterior chamber or iris-fixated IOLs can be implanted, or, alternatively, a posterior chamber IOL can be fixated in the ciliary sulcus using transscleral suturing or gluing. Scleral-sutured IOLs have been popular in the past; however, to avoid the intraoperative and postoperative suture-related problems, Gabor and Pavlidis developed a sutureless technique for sulcus fixation of posterior-chamber IOL using permanent incarceration of the haptics in a scleral tunnel parallel to the limbus9. This method offers postoperative axial stability of the IOL while avoiding suture-related problems. This method combines the control of a closed-eye system with the postoperative axial stability of the posterior chamber IOL. This technique has an advantage in that it can be performed in the presence of significant structural abnormalities of the anterior chamber and that it mitigates many of the adverse outcomes associated with AC IOL’s, iris fixated IOL’s and sutured scleral fixated IOL’s.
Removal of the crystalline lens deprives the eye of the stabilizing effect of the lens-zonule barrier. When the eye moves, it acquires kinetic energy from its muscles and attachments and the energy is dissipated to the internal fluids as it stops. Thus pseudophacodonesis is the result of oscillations of the fluids in the anterior and posterior segment of the eye. The oscillations, initiated by movement of the eye, result in shearing forces on the corneal endothelium which may result in damage. Similar motion of the vitreous causes shearing forces which may damage the retina10,11.In sutured scleral fixated IOL, there is increased chance of pseudophacodonesis due to torsional instability of ciliary body-suture-haptic attachment while in scleral tucking of haptic there is less chance of torsional instability due to rigid ciliary body-haptic-optic attachment12.
In this observational study, 50 cases were taken. Out of 50, 24 were aphakic due to complicated cataract surgery & 2 were aphakic after ICCE. These cases underwent deep core anterior vitrectomy through 23-gauge pars plana route with scleral fixation in same sitting. During anterior vitrectomy infusion continued through anterior chamber maintainer and a single pars plana incision 3.5 mm behind the limbus was made. This allowed the flow to move in one direction from anterior to posterior making removal of vitreous more efficient. Rest of the cases included dropped IOL (4), nucleus drop (5), subluxated cataractous lens (4), traumatic posterior dislocated crystalline lens (3), cortical matter in vitreous (1), operated limboscleral tear with subluxated cataractous lens (1), subluxated IOL (1), subluxated traumatic cataract with IOFB (2), traumatic cataract with IOFB (1), traumatic posterior dislocated IOL (1), traumatic subluxated IOL with inferior retinal dialysis (1). In these cases 23- gauge primary pars plana vitrectomy with 360° endolaser was done. Silicon oil was injected in required cases. Then after 4 weeks SFIOL was implanted. In silicon filled eye SFIOL was implanted after silicon oil removal. After vitrectomy one case with traumatic cataract with IOFB developed CME which was treated medically and followed up routinely with OCT & SFIOL was implanted when CME was resolved completely.
Change in corneal curvature & astigmatism due to this technique was found insignificant. P-value for K1 was 0.6324, for K2 was 0.4556 & for astigmatism 0.0510. It signifies that this scleral tunnel do not interfere in corneal topography & astigmatism.
On day 1 all IOL were well centered, there were 2(4%) cases of corneal edema & mild anterior chamber reaction due to surgical manipulations, which got resolved on next follow up. Because of this hazy media in 2 cases, OCT could not be taken on day 1. On day 7, there were 3 (6%) cases of raised IOP, for which antiglaucoma drugs started and after one week IOP was well controlled. Later antiglaucoma stopped and IOP was within normal limits. There was also 2 (4%) case of decentration with exposed haptic on day 7. Haptic was placed back in scleral tunnel & IOL was recentered surgically. At 3 month follow up, there was 1 (2%) case of CME which was treated medically & 1 (2%) case of dislocation for which IOL was recentered surgically. On last follow up, all cases have well centered IOL. So out of 50, there were 2 cases of decentration, 1 case of CME, 3 cases of raised IOP and 2 cases of corneal edema.
Because of the overall diameter of these IOLs, we did not observe increased forces to the sclera. Scleral tunnels are well known from cataract surgery, and we would not expect scleromalacia to occur except, possibly, in cases of pre-existing inflammation (eg, Scleritis, episcleritis, rheumatoid arthritis, herpes zoster ophthalmicus) 13.
This technique also minimizes intraoperative maneuvers, which could reduce the risk for intraoperative trauma. Using a foldable IOL and (preferably) implanting it using an injector keep the incision small and prevent higher surgically induced astigmatism. Furthermore, the technique can be performed with a standard 3-piece PC IOL without need for special haptic architecture or haptic preparation or for storage or ordering special IOLs for rare indications.
It has been shown that the overall length (12.5–14.0 mm) of the IOL helps ensure firm, stable fixation at the posterior chamber behind the iris, where the average diameter in emmetropic eyes is approximately 13.0 mm. In addition, the large optics lowers the risk of clinically significant postoperative decentration. Since the overall diameter of the routine IOL is about 12–13 mm, with the haptic being placed in its normal curved configuration and without any traction, there is no distortion or change in shape of the IOL optic12. Externalization of the greater part of the haptic along its curvature stabilizes the axial positioning of the IOL and thereby prevents IOL tilt14. Intraoperative IOL centration is possible due to adjustments made to the final intrascleral position of the haptics. Sulcus fixation of single-piece IOLs is not popular owing to postoperative complications like pigment dispersion, iris transillumination defects, dysphotopsia, elevated IOP, intraocular hemorrhage and cystoid macular edema. This is due to the fact that bulky single-piece haptics are large and thick enough to contact the posterior iris when placed in the sulcus. Also, the haptics are planar rather than angulated and therefore do not vault the optic posteriorly from the iris15.
Although the eyes in our study were complex with numerous pre-existing ocular conditions and some postoperative complications occurred, the mean BCVA after surgery was statistically significantly better than before surgery. Based on these findings, we believe our technique simplifies scleral fixation in aphakic patients. The scleral fixation technique has evolved over time, with one of the greatest changes being the use of foldable IOLs. This makes it possible to perform the entire procedure through small self-sealing incisions. This has the intraoperative advantage of having a well-formed globe throughout the surgery. It eliminates iris prolapse during IOL insertion and wound suturing and significantly decreases surgical time. This foldable IOL has postoperative advantages of having fewer complications associated with larger wounds, such as postoperative wound leak and shallow anterior chamber, as well as decreases the astigmatism.
We believe this method of PCIOL implantation is appropriate for eyes with deficient or absent posterior capsule and this can be performed easily with the available IOL designs, instruments and with less surgical time. However, evaluation of the clinical importance of the technique requires a clinical study with greater number of patients and longer duration follow up to judge the long term functional and anatomical results of the procedure.
Based on our current experience and published results, sutureless PC IOL implantation is an effective alternative in eyes with deficient capsule support.
References-
1.Apple, DJ, Mamalis, N, Loftfield, K et al, Complications of intraocular lenses. A historical and histopathological review. Surv Ophthalmol. 1984;29:1–54.
2.Lundström M, Brege KG, Florén I, Lundh B, Stenevi U, Thorburn W.: Postoperative aphakia in modern cataract surgery: part 2: detailed analysis of the cause of aphakia and the visual outcome.J Cataract Refract Surg. 2004 Oct;30(10):2111-5.
3.Alpar J-“Present state of management of aphakia. Future of spectacles and contact lenses”.:Indian J Ophthalmol. 1989 Apr-Jun;37(2):54-7
4.Dabezies OH Jr., Defects of vision through aphakic spectacle lenses. Ophthalmology. 1979 Mar;86(3):352-79.
5.Ferris RL., Complications associated with aphakic contact lenses.Ophthalmology. 1979 Jun;86(6):1120-3.
6.Por YM, Lavin MJ. Techniques of intraocular lens suspension in the absence of capsular/zonular support. Surv Ophthalmol 2005; 50:429–462
7.Apple DJ, Brems RN, Park RB, Norman DK, Hansen SO, Tetz MR, Richards SC, Letchinger SD., Anterior chamber lenses. Part I: Complications and pathology and a review of designs. J Cataract Refract Surg. 1987 Mar; 13(2):157-74.
8.Mervi Bergman, Leila Laatikainen. Long-term evaluation of primary anterior chamber intraocular lens implantation in complicated cataract surgery International Ophthalmology1996, Volume 20, Issue 6, pp 295-299.
9.Gabor SGB, Pavlidis MM. Sutureless intrascleral posteriorChamber intraocular lens fixation. J Cataract Refract Surg2007; 33:1851–1854
10.Jacobi KW, Jagger WS.Physical forces involved in pseudophacodonesis and iridodonesis.Albrecht Von Graefes Arch KlinExp Ophthalmol. 1981;216(1):49-53.
11.Binkhorst CD.Corneal and retinal complications after cataract extraction. The mechanical aspect of endophthalmodonesis. Ophthalmology. 1980 Jul;87(7):609-17.
12.Narang P, Beiko G, Ohta T, Agarwal A. Modifications in the glued IOL technique. In: Agarwal A, Ed, Glued IOL: Glued Intrascleral Haptic Fixation of a PC IOL. New Delhi, India, JaypeeBrothers, 2013; 88–96
13.Mamalis N, Johnson MD, Haines JM, Teske MP, Olson RJ. Corneal-scleral melt in association with cataract surgery and intraocularlenses: a report of four cases. J Cataract Refract Surg1990; 16:108–115
14.Teichmann KD, TeichmannI A. The torque and tilt gamble.J Cataract Refract Surg 1997;23:413-8.
15.David F, Chang MD, et al: Complications of sulcus placement of single-piece acrylic intraocular lenses. Recommendations for backup IOL implantation following posterior capsule rupture. J Cataract Refract Surg 2009;35:1445-1458.