W. Dr. Anjum Iqbal Mazhari,
M16354, Dr. Ruchi Shukla, Dr. Puneet Mahajan
AnjumMazhari MS1, Puneet Mahajan DO1, Ruchi Shukla MS1
1Indira Gandhi Eye Hospital & Research Centre, Lucknow, India
Introduction:
Ocular surface squamous neoplasia (OSSN) encompasses a broad spectrum of neoplastic squamous epithelial abnormalities, including squamous dysplasia, conjunctival intraepithelial neoplasia (CIN), and invasive squamous cellcarcinoma (SCC).1, 2It represents the most common nonpigmented tumor of theocular surface.
These neoplastic conditions can affect the conjunctiva and the corneal surface, and occasionally invade into the globe, orbit, andthe nasolacrimal system.1–3
Complete tumor resection to avoid destructive local invasion, recurrence, and metastasis is an essential issue in the treatment of OSSN. Even with clean rmargins on pathology specimens, recurrences of up to 33% have been reported.6 As a result, adjuvant therapies are often performed with excision, including cryotherapy or topical chemotherapy, with reduction in the rates ofrecurrence.7-9
Chemotherapeutic agents used for treatment of OSSN include Mitomycin C, 5-Fluorouracil, and Interferon (IFN)α2b, all of which have been shown to be effective.10-12
Reconstruction of large excised areas ensuring both good functional and cosmetic results is as much important and can be very challenging. When the wound cannot be closed primarily, several surgical techniquesmight be used for the management of these tissue defects. These methods, including amniotic membrane transplantation (AMT), transpositional or free flap conjunctival autografting, limbal transplantation, and oralmucosa transplantation have their advantages as well as limitations.13In cases with wide defects, excessive harvest of these tissues may result in complications at the donor and recipient site that may cause cosmetic problems, patient discomfort and even visual dysfunction.14, 15
The amniotic membrane promotes epithelization by functioning as a substrate for growth of epithelial cells. It also serves as an anti-angiogenic, anti-inflammatory, and anti- fibrotic agent with the help of its structural and biochemicalcomposition.16
In previously conducted studies amniotic membrane transplantation has been shown to be an effective technique for the management of ocular surface reconstructions following the excision of conjunctival tumors.17, 18
In developing countries amniotic membrane availability remains a major issue hence we decided to assess the safety and clinical outcomes in patients over a period of 3 years who has undergone excision biopsies of ocular surface squamous neoplasia (OSSN) and the big resultant conjunctival defects were closed with small autograft by a newer ‘Step Ladder Pattern’ pulling and suturing technique.
Materials and methods
8 patients (8eyes) who underwent excision of OSSN followed by conjunctival autograft were enrolled in the study. Surgeries wereperformed in the same clinic bythe same surgeon.
During each follow-up visit, slit-lamp biomicroscopy and fluorescein staining were performed, noting the integrity,smoothness of the ocular surface, any signs of any complications (inflammation, scarring,vascularization, and corneal opacities), and recurrences.
Treatment results were defined as successful if complete healing of the surgical wound was achieved and ifthere were no clinically significant complications or recurrences of the tumor.
All operations were performed under local anesthesia. All tumors were resected intact, using the ‘no touch’technique with at least 3-4 mm normal-looking conjunctiva (safe margins).19
All excised tissues were sent forhistopathologic evaluation to the pathology department.Double freeze–thaw cryotherapy was applied to the remaining conjunctival margins. For tumors invading thecornea before tumor excision corneal epitheliectomy with absolute alcohol application was performed.
The conjunctival defects were reconstructed up to the limbus with closing small (4-6 mm) conjunctival autografts. The defects were pulled in a step ladder pattern to avoid restriction of eyeball movements postoperatively and secured with the autograft by 8-0 vicryl/10-0 Nylon sutures.While suturing, attention was paid to avoid tension on the autograft. Topical corticosteroid and antibiotic eye drops were used four times daily for a month. Two interrupted cycles of 0.04 % Mitomycin C eye drop were given.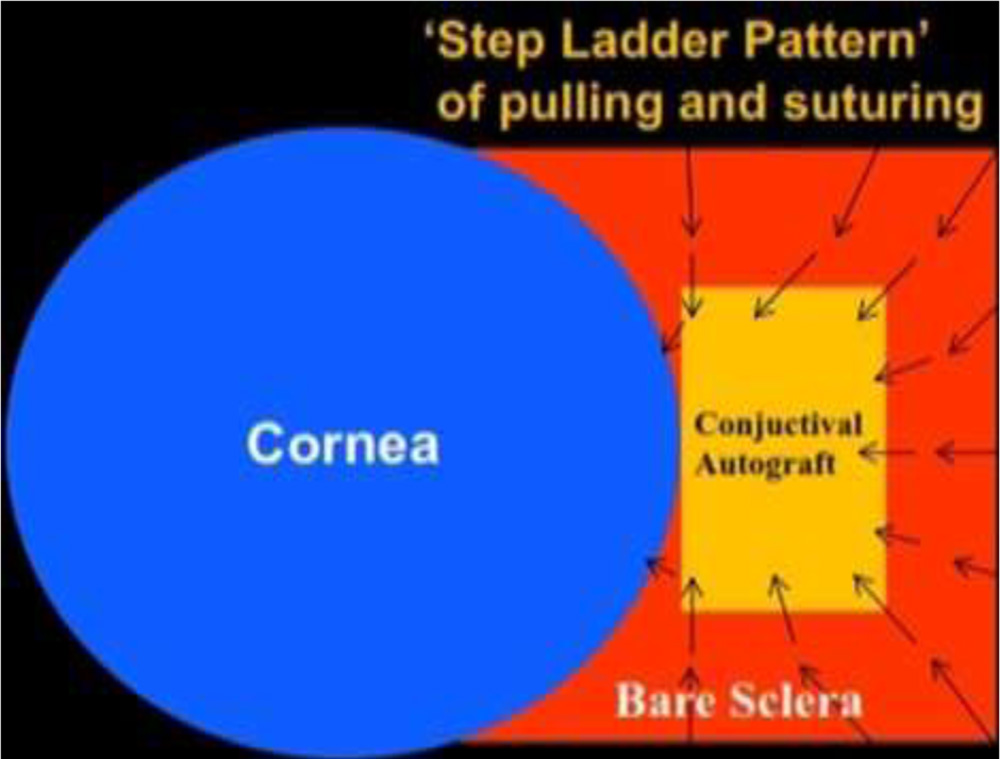
Results
The mean age of the 8 patients (2 female, 6 male patients) was 42.0±10.90 (range 18-54) years. The right eye was affected in 5, and the left eye was affected in 3 patients. All tumors were primary and did not receive any prior treatment. None of the patients had any local invasionsto the orbit or any local lymph node metastasis at the time of surgery.Complete tumor removal confirmed using histopathology was achieved in all cases (100%). Theaverage diameter of the base of the tumors was 9.50 ± 1.41 (range, 8-12) mm. bulbarconjunctiva was involved in allcases. The tumors invaded the limbal area in 7 cases (87.5 %). The mean extent of the limbal involvement was4±2.5 (range, 2–8) clock hours.Pathologic diagnosis of the tumors were squamous dysplasia (one eye), CIN (three eyes), andSCC (four eyes).No surgical complications were observed. Postoperatively, the autograft completely covered the surgical defect of theocular surface in all cases.Transient signs of mild discomfort and foreign body sensation lasted for 2–3weeks.The mean follow-up time was 26.87 ± 10.84 (range, 15–42) months.At the last follow-up visit, the patients did not report any symptoms associated with the surgery and were satisfied with the cosmetic appearance of their eyes.In all cases, a final slit-lamp examination with fluorescein staining showed complete epithelization of the tissue defect; a noninflamed and wet surface of conjunctiva and cornea was observed.No recurrence was observed in a follow-up time of 26.87 ± 10.84 (range, 15–42) months.
Discussion
Surgical excision of OSSN larger than 10-mm base diameter might result in wide tissue defects that cannot be closed primarily.
These defects require reconstruction with adjunctive methods, such as transpositional conjunctival flap, free conjunctival graft from the opposite eye, and/or oral mucosal grafts,amniotic membrane transplantation.
Thick mucosal grafts, such as buccal tissue, are associated with an unsatisfactory cosmetic result, as they occupy large spaces in the fornix, may shrink with time, may mask regrowth of the underlying tumor, and lead to a non-conjunctival epithelial morphology.20
Amniotic Membrane Transplantation (AMT) offers an advantage over buccal mucosal autografts, which invariably result in a non-conjunctival epithelial morphology. The AMT reconstructed conjunctival surface retains a normal conjunctival epithelial phenotype as shown by impression cytology.21
The high success rates of Amniotic membrane in ocular surface reconstruction are because of promoted epithelization, anti-inflammatory, antifibrotic, and antiangiogenic effects, and low immunogenecity.22
On comparison with amniotic membrane the main handicap of autologous grafts and flaps is the shortage of the utilizable tissue.
Moreover, in case of conjunctival grafts, harvest of adequately sized conjunctival autografts may result in donor-site morbidity, including scarring, secondary granulation tissue, symblepharon,restricted ocular/eyelid motility, and partial or total limbal stem cell deficiency.20
But,if conjunctival autograft is used to cover the defect area it presents a benefit of having a higher likelihood of promoting the restoration of a normal appearance.23
Despite the advantages of amniotic membrane we went for closing the resultant big conjunctival defects by a small autograft by ʿStep Ladder Pattern’pulling and suturing of conjunctival margins and securing it with the conjunctival autograft.
In contrast to small autografts, our new technique has an advantage over them in showing no restriction of eye motility and symblepharon formation.
Fresh Amniotic membrane poses a risk of disease transmission, whereas the drawback with preserved amniotic membrane is the need for a -70° refrigerator, which precludes its use outside big institutions.24
Therefore in third world countries and remote locations, use of conjunctival autograft can be done with the help of our technique.
Although, amniotic membrane transplantation is the first choice for closing the large conjunctival defect but in cases of limited resources i.e. less availability of amniotic membrane as well as due to financial constraints,our technique of using conjunctival auto graft is quite effective.
Due to shortage of literature on closing defects with autograft we compared our findings with amniotic membranetransplantation.
Our findings in terms of healing were consistent with earlier reported results of several case series of AMT after conjunctival tumorexcision.25
In our study, no surgical complications were observed. The postoperative period of milddiscomfort and inflammation was short and effectively managed with topical steroids.
Successful ocular surfacereconstruction and complete healing were achieved in all eyes.
No surface or intra-ocular inflammation nor persistent epithelial defect or fluorescein staining were recorded in any eyes during the follow-up period.
No recurrence was observed in any eyes.
As a conclusion, conjunctival autograft used with our ʿStepLadderʾtechniquepermits more generous margins with a healthy ocular surface in extensiveconjunctival OSSN.
It is an effective method of reconstruction following OSSN excision, cryotherapyof surgical wound margins, and cornealepitheliectomy with absolute alcohol application.
In most cases, complete healing of the ocular surface can be achieved without any clinicallysignificant complications and with good cosmetic and functional results.
Hence, our study offers an alternative surgical management for ocular surface neoplasias.
Limitations:
The size of our sample was not large enough to conclude regarding recurrence after surgery. New studies including an additional number of patients and a longer follow up are needed for further conclusions.
References:
- Shields JA, Shields CL. Premalignant and malignant lesions of the Conjunctival epithelium. In: Shields JA, Shields CL (eds). Eyelid, Conjunctival, and Orbital Tumor: An Atlas and Textbook. LippincottWilliams&Wilkins Co: Philadelphia, PA, USA, 2008, pp 286–305.
- Kiire CA, Srinivasan S, Karp CL. Ocular surface squamous neoplasia. IntOphthalmolClin 2010; 50: 35–46.
- Shields CL, Demirci H, Karatza E, Shields JA. Clinical survey of 1643 melanocytic and nonmelanocytic conjunctival tumors. Ophthalmology 2004; 111: 1747–1754.
- Shields CL, Shields JA. Tumors of the conjunctiva and cornea. SurvOphthalmol 2004; 49: 3–24.
- Napora C, Cohen EJ, Genvert GI, Presson AC, ArentsenJJ,Eagle RC et al. Factors associated with conjunctival intraepithelial neoplasia: a case control study. Ophthalmic Surg 1990; 21: 27–30.
- Tabin G, Levin S, Snibson G, et al. Late recurrences and the necessity for long-term follow-up in corneal and conjunctival intraepithelial neoplasia. Ophthalmology 1997;104:485–92.
- Peksayar G, Altan-Yaycioglu R, Onal S. Excision and cryosurgery in the treatment of conjunctival malignant epithelialtumours. Eye (Lond) 2003;17:228–32.
- Siganos CS, Kozobolis VP, Christodoulakis EV. The intraoperative use of mitomycin-C in excision of ocular surfaceneoplasia with or without limbal autograft transplantation.Cornea 2002;21:12–6.
- Midena E, Angeli CD, Valenti M, et al. Treatment of conjunctival squamous cell carcinoma with topical 5-fluorouracil. Br J Ophthalmol 2000; 84:268–72.
- Frucht-Pery J, Sugar J, Baum J, et al. Mitomycin C treatment for conjunctival-corneal intraepithelial neoplasia: a multicenter experience. Ophthalmology 1997;104:2085–93.
- Galor A, Karp CL, Chhabra S, et al. Topical interferon alpha 2b eye-drops for treatment of ocular surface squamousneoplasia: a dose comparison study. Br J Ophthalmol 2010; 94:551–4.
- Yeatts RP, Ford JG, Stanton CA, Reed JW. Topical 5-fluorouracil in treating epithelial neoplasia of the conjunctiva andcornea. Ophthalmology 1995;102:1338–44.
- Asoklis RS, Damijonaityte A, Butkiene L, MakselisA,Petroska D, Pajaujis M et al. Ocular surface reconstruction using amniotic membrane following excision of conjunctival and limbal tumors. Eur J Ophthalmol 2011; 21: 552–558.
- Neuhaus RW, Baylis HI, Shorr N. Complications at mucous membrane donor sites.Am J Ophthalmol 1982;93(5):643-646
- Vrabec MP, Weisenthal RW, Elsing SH. Subconjunctival fibrosis afterconjunctival autograft. Cornea 1993;12(2):181-183
- Dua SH, Azuara-Blanco A. Amniotic membrane transplantation. Br J Ophthalmol 1999; 83: 748–752.
- Espana EM, Prabhasawat P, Grueterich M, Solomon A, Tseng SC.Amniotic membrane transplantation for reconstruction after excision oflarge ocular surface neoplasias.Br J Ophthalmol 2002;86(6):640-645
- Asoklis RS, Damijonaityte A, Butkiene L, Makselis A, PetroskaD,Pajaujis M, Juodkaite G. Ocular surface reconstruction using amnioticmembrane following excision of conjunctival and limbaltumors.Eur J Ophthalmol2011;21(5):552-558
- Shields JA, Shields CL, DePotter P. Surgical management of conjunctival tumors: the 1994 Lynn B. McMahan Lecture.Arch Ophthalmol 1997; 115: 808–815.
- Gunduz K, Ucakhan OO, Kanpolat A, Gunalp I. Nonpreserved human amniotic membrane transplantation for conjunctival reconstruction of extensive ocular surface neoplasias. Eye 2006; 20: 351–357.
- Prabhasawat P, Tseng SCG. Impression cytology study of epithelial phenotype of ocular surface reconstructed by preserved human amnioticmembrane. Arch Ophthalmol 1997; 115:1360–7.
- Dua HS, Gomes JA, Kinng AJ, Maharajan VS. The amnioticmembrane in ophthalmology. SurvOphthalmol 2004; 49:51–77.
- Rahman L,BaigMA,IslamQ.Prevention of pterygium recurrence by using intra operative5 flourouracil,Pakistan Armed Forces Medical J.2008;1:23
- Sangwan VS, Burman S, Tejwani S, Mahesh SP, Murthy R. Amniotic membrane transplantation: A review of current indications in the management of ophthalmic disorders. Indian J Ophthalmol 2007;55:251-60
- Tseng SCG, Prabhasawat P, Lee SH. Amniotic membrane transplantation for conjunctival surface reconstruction.Am J Ophthalmol 1997; 124: 765–774.