Dr. Bhupesh, B12314
Microbial Keratitis in Stevens – Johnson syndrome: Clinico-Microbiological Profile Study
Bhupesh Bagga FRCS1, Swapna Reddy MD2, Virender Singh Sangwan MD1, Savitri Sharma MD2
1 Tej Kohli Cornea Institute, L.V.Prasad eye institute Hyderabad
2Jhaveri Microbiology Centre
L.V.Prasad eye institute Hyderabad
Corresponding Author
Bhupesh Bagga F.R.C.S.
Consultant
Tej Kohli Cornea Institute
L.V.Prasad Eye Institute Road No.2Banjara Hills
Hyderabad 500034
India
Abstract
Purpose– To study the clinico-microbiological profile of microbial keratitis in Stevens-Johnson Syndrome (SJS)
Study design– Case Series
Participants– Patients of SJS who developed microbial keratitis
Methods– Medical records and microbiological data of patients with SJS who developed microbial keratitis from January 1991 to December 2012 were reviewed. We analysed the type of causative organisms and their antibiotic susceptibility along with clinical pattern and response to medications in this group of patients.
Main Outcome Measure–
Clinical and microbiological profile of microbial keratitis
Results–
We reviewed 70 eyes of 62 patients seen between January 1991 and December 2012. Positive microbiological culture results were obtained in 45 eyes (64.3%). Isolated bacterial infections were noted in 27/45 cases (60%) while isolated fungal growth was seen in 1/45 case (2.2%). Polymicrobial infections were noted in 17/45 cases (37.8%). Out of 59 bacterial growths 21 (35%) were Staphylococcus spp. which were the most common. But interestingly incidence of Fungal keratitis (7%) was less compared to patients without SJS (38%). The occurrence of microbial keratitis was seen more commonly in 31/70 (45%) earlier phase of SJS (<3months) than late (median duration 6 months). Margins of ulcer were rounded, heaped up and well defined in 28/70 (40%) eyes. Duration of onset of infection to presentation to clinic ranged between 3 days to 2 weeks. Twenty eight eyes (40%) needed additional treatment (tarsorraphy, epilation, tissue adhesive application, and amniotic membrane grafting or punctal cautery) for resolution along with antibacterial agents. Corneal ulcers resolved in 40 /70 eyes (57%). Average time of resolution was 25 days.
Conclusion–
Microbial keratitis in SJS patients is different from patients without SJS in presentation and the response to medications. It requires multidisciplinary approach for healing.
Introduction
Stevens-Johnson syndrome (SJS) comprises of generalized exanthematous reaction which involves the ocular surface both in acute and chronic stages. It is an autoimmune condition presenting as severe cicatrising conjunctivitis. In the chronic phase of SJS most of the co-morbidities are due to associated lid margin abnormalities and chronic adnexal inflammation. Stevens-Johnson Syndrome can be incited by various agents. Ocular complications due to SJS sequelae have been studied previously1. Grading of SJS2 depends on ocular involvement. Frizon et al3 studied the conjunctival flora of SJS patients and their antimicrobial susceptibility. Ormerod et al4 had studied corneal infections in mucosal scarring disorders and Sjögren’s syndrome. In that study patients with Ocular Cicatricial Pemhigoid, SJS, Graft versus Host Disease were included. In the present study we describe the clinico-microbiological profile of patients with SJS who developed microbial keratitis. We believe that the clinical and microbiological spectrum of infective keratitis in patients with SJS may be different than patients without SJS and also the clinical response to treatment may be different due to use of prophylactic antibiotics along with use of long term steroids and other forms of immunosuppression. To the best of our knowledge this is the largest study of such a group of patients which also highlights the multidisciplinary approach towards such cases. We have compared our results in patients with SJS to the historical data available in the literature for patients without SJS.
Methodology-
This is a retrospective analysis of medical records of all patients with a diagnosis of both SJS and microbial keratitis. The study was approved by Institute Review Board of L.V.Prasad Eye Institute. We reviewed the records from Jan 1991 to Dec 2012. The hospital records were reviewed to obtain a detailed demographic data, laterality and duration of initial insult to the time of presentation. We also collected the data of clinical characteristics of corneal ulcers along with adnexal involvement. The cases were classified into 3 grades, depending on the associated conjunctival involvement, lid margin abnormalities, and severity of dry eye. Corneal scrapings were obtained from the patients according to the standard institutional protocol. Every corneal scraping was subjected to a direct microscopic examination, culture and antibiotic susceptibility testing. Microscopic examination included Gram stain, and potassium hydroxide with calcofluor mount. The samples were inoculated directly onto 5% sheep blood agar, chocolate agar, Sabouraud dextrose agar, potato dextrose agar, brain heart infusion broth and thioglycollate broth as a part of the standard institutional protocol. SDA and PDA were incubated at 25-27°C for 2 weeks to detect fungal growth, while the remaining media were incubated at 35-37°C for 1 week for the detect of bacterial growth.
All bacterial isolates were identified to the species level using the Vitek II compact system, while the fungal isolates were identified by gross morphology and microscopic examination of lactophenol cotton blue mount. Bacterial isolates were further subjected to antibiotic susceptibility testing by Kirby Bauer disc diffusion method.
Results-
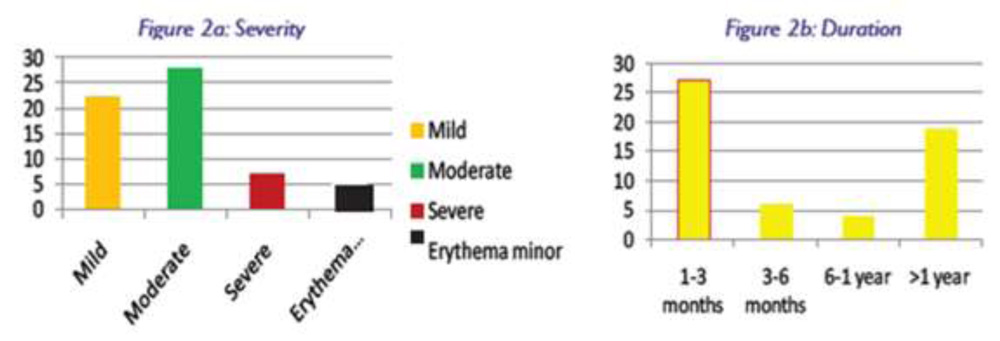
We reviewed the records of 62 patients (70 eyes). Their ages ranged from 4 to 65 years (median age 25 years). There were 33 males and 29 females. Cases of SJS were divided into 4 grades (Fig.2a). Most common drugs responsible for SJS were sulphur containing medications followed by phenytoin. The occurrence of microbial keratitis was seen more commonly (45%) in earlier phase of SJS (<3months) than late (median duration 6 months) (Fig.2b). Duration of onset of infection to presentation to clinic varied between 3 days to 2 weeks . There were 13 (N=21) patients who presented with bilateral microbial keratitis. Median visual acuity at presentation was 1.6 LogMAR units in 57(92%) patients. Corneal ulcers were graded into 3 groups based on their sizes. Group 1(39%) comprised of less than 3 mm size, Group 2 (45%) ulcer size was between 3 to 6 mm, and Group 3 (29%) ulcer size was more than 6 mm. There were nine (16.5%) cases who presented with perforated corneal ulcer. Margins of ulcer were rounded, heaped up and well defined in 28(45%) eyes. Deep stromal vessels were noted in 12(19%) eyes.
Positive microbiological culture results (Fig.4) were obtained in 45 eyes (64.3%), while 25 (35.7%) were sterile. Infection with single bacterial species was noted in 27/45 cases (60%). Infection with single fungal species was seen in 1/45 case (2.2%). Polymicrobial infections were noted in 17/45 cases (37.8%). Out of 59 (Tab.1) bacterial isolates Staphylococcus spp. was the most common (35%) bacterial species. There were 5 cases of Fungal keratitis out of which 3 grew Candida and 1 each grew Aspergillus and Cladosporium species. Susceptibility of Gram positive and negative bacteria are shown in Table 2 (a&b). As an initial treatment topical Fortified Cefazolin (5%) was started in 17 eyes, Ciprofloxacin 0.3% in 25 eyes, Gentamicin 0.3% in 7 eyes in intensive medication dose (every hour). In 12 eyes, Choramphenicol 0.5% was started 4 times in a day dose. Ophthalmic lubricants were started as an initial treatment in 12 eyes. Steroids were added in 7 eyes after seeing the initial response of treatment for 2-3 days. Twenty eight eyes (Fig.5) needed additional treatment for resolution as well as to give tectonic support due to associated corneal thinning and stromal melt. Tissue adhesive was applied in 9 cases, 8 cases needed tarsorraphy while amniotic membrane graft was applied in 5 cases. Punctal cautery and epilation were done as an additional procedure to treat dry eye, trichiasis and distichiasis. While penetrating keratoplasty was performed in 3 eyes, 1 eye was eviscerated. There were 40 (57%) corneal ulcers which improved with the help of all the measures used along with antibacterial agents and healed. Average time of resolution was 25 days. In remaining eyes, 20 got worsened, 5 remained status quo and 5 were lost to follow up. In one case (Fig.6) it took 35 days for infection to resolve.
Discussion-
This study demonstrated that clinical profile and outcome of microbial keratitis in Stevens-Johnson Syndrome is mutifactorial, as it not only depends on the organism and its virulence but also the adnexal tissue health. Most commonly it occurs either very early (1-3 month) or late (> 1year) stages of SJS. In acute SJS, this can be explained by poor epithelium, increased inflammation, poor blink rate along with exposure keratopathy along with use of steroids, while in chronic stages1 it is associated with lid margin keratinisation, distichiasis, entropion or ectropion and severe dry eye. Microbial keratitis in normal conditions is more commonly seen due to bacterial causes5 which is similar to our SJS group. Most common organism is Staphylococcus species which is similar to other epidemiological studies from our institute.6. But interestingly incidence of Fungal keratitis (7%) is less compared to patients without SJS (38%). This can be explained by the fact the most common cause of microbial keratitis is trauma with vegetative matter and fungal infection. Regarding antimicrobial susceptibility these organisms have increased resistance. Drug sensitivity of Gram positive bacteria for Cefazolin, Chloramphenicol, Ciprofloxacin and Gentamicin in our study was 76.5%, 72.5%, 33.4%, and 47.1% respectively while previously6 it was reported to be 92.3, 75.5%, 70.2% and 68.8% respectively. For Gram negative bacteria the drug sensitivity for Gentamicin, Ciprofloxacin, and Chloramphenicol noted in our study was 75%, 37.5% and 50% respectively while the same was 86.9%, 85.8% and 27.3% in previous reports6. The susceptibility for Ciprofloxacin is significantly less in the study group. This data can suggest the empirical first line medication for microbial keratitis in SJS. Healing of corneal ulcers depends on the etiological event and ocular adnexal health. The time to resolve bacterial keratitis in otherwise healthy eyes is 3 to 7 days need to find the references while in patients with SJS (study group) it responded slowly and became persistent non-healing epithelial defects and responded in an average 25 days (range14 to 55 days). This information can be clinically useful in a manner that changing medication or increasing frequency of antibiotics will only add the toxicity on the ocular surface. Rather we should take the measures to improve the ocular surface. Extrapolation of the data for drug sensitivity and comparing with the previous study 5, 6 is a limitation of the present study due to different cohort and time period of the two studies, as antibiotic susceptibility per se is changing since 2 decades. Additional measures taken to improve the ocular surface were primarly targeting the healing of epithelial defect. Tarsorraphy7 (paramedian or central) had been described as one of the important,t this needs a multidisciplinary approach targeting not only the organisms but also towards dry eye, lid margin treatment, inflammation and associated exposure.
References-
- Di Pascuale MA, Espana EM, Liu DT et al. Correlation of Corneal Complications with Eyelid Cicatricial Pathologies in patients with Stevens–Johnson Syndrome and Toxic Epidermal Necrolysis Ophthalmology 2005;112:904–12.
- Sotozono C, Ang LP, Koizumi N, et al. New Grading System for the Evaluation of Chronic Ocular Manifestations in Patients with Stevens–Johnson Syndrome. Ophthalmology 2007; 114:1294–302.
- Frizon L, Araújo MC, Andrade L, et al. Evaluation of conjunctival bacterial flora in patients with Stevens – Johnson syndrome. CLINICS 2014;69:168-72
- Ormerod LD, Fong LP, Foster CS. Corneal infections in Mucosal Scarring Disorders and Sjogren’s syndrome. Am J Ophthalmol 1988; 105: 512-18
- Gopinathan U, Sharma S, Garg P, Rao GN. Review of epidemiological features, microbiological diagnosis and treatment outcome of microbial keratitis: experience of over a decade. Indian J Ophthalmol 2009;57:273-9
- Sharma S, Kunimoto DY, Rao N T, et al. Trends in antibiotic resistance of corneal pathogens: Part II. An analysis of leading bacterial keratitis isolates, Indian J Ophthalmol.1999;47: 101-09
- .Pakarinen M, Tervo T, Tarkkanen A Tarsorraphy in the treatment of persistent corneal Acta Ophthalmol Suppl.1987;182:69-73.
Figure legends
- 1 a) shows bar diagram depicting severity of SJS (a) in this group of patients and duration (b) of SJS showing the time gap between the onset of SJS and time of presentation to clinic.
- Figure 2 Figure 3 has pie chart showing percentages of adjuvant treatment done in addition to the use of antimicrobials
- Fig.2
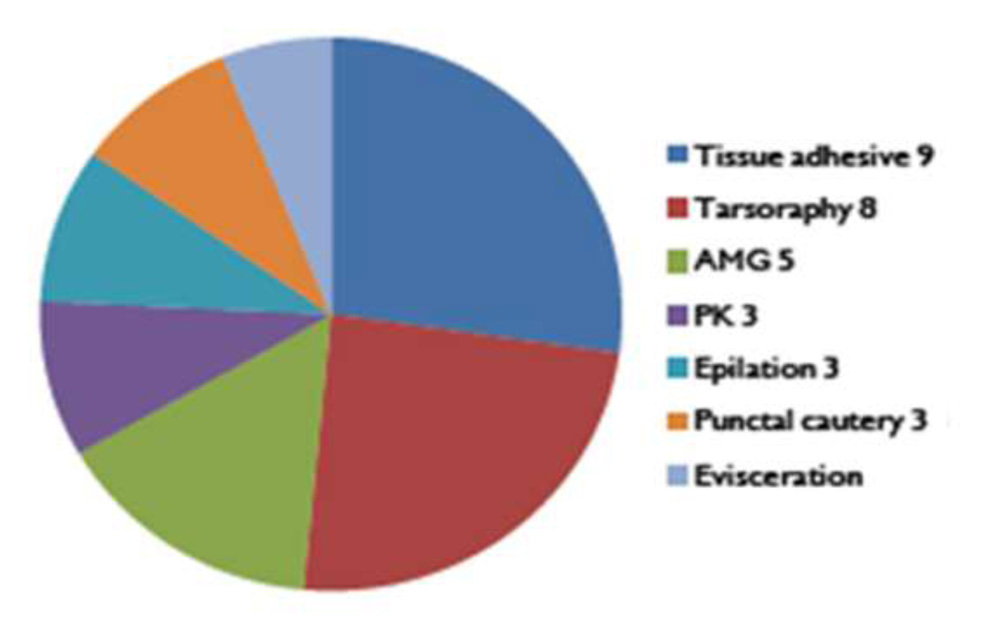
Table 1: Types of bacterial species isolates in patients with microbial keratitis
| Bacteria species grown | N |
| Staphylococci | 21 (35%) |
| Streptococci | 14 (24%) |
| Corynebacteria | 15 (25.5%) |
| Brevibacterium | 1 |
| Pseudomonas aeruginosa | 4 |
| Escherichia coli | 3 |
Table 2: Antibiotic Susceptibility of Gram Positive (A) and Gram Negative bacteria (B)
| Gram Positive Bacteria (A) | Gram Negative Bacteria (B) | ||
| Antibiotic | Susceptible% | Antibiotic | Susceptible% |
| Vancomycin | 100 | Aminoglycosides
|
6/8 (75%), |
| Cefazolin | 76.5 | Ceftazidime
|
5/8 (62.5%), |
| Chloramphenicol | 72.6 | Chloramphenicol | 4/8 (50%) |
| Ciprofloxacin | 33.4 | Gatifloxacin
|
4/8 (50%) |
| Gentamicin | 47.1 | Ciprofloxacin
|
3/8 (37.5%). |