Dr. Jayanta Kumar Das, D07473, Dr. (Mrs ) Kasturi Bhattacharjee
Chief and Presenting Author: Dr.Jayanta Kr. Das (AIOS Number: D07473)
Co Author: Dr.KrishnaGogoi
Dr.KasturiBhattacharjee
Dr.Diva Kant Misra
Affiliation: Sri SankaradevaNethralaya
We have no financial interests or relationships to disclose
Abstract:
Purpose:
To identify the most common route of infection in cases of chronic Dacrysocystitis. Methods:A prospective analysis of conjunctival, lacrimal sac and nasal mucosal content of 300 patients between Jan 2012 to Jun 2015.Three specimens were obtained, from anatomical opening of NLD at nose, from conjunctiva and lacrimal sac during DCR of the effected side for culture. Results: Growths were observed in 228(76%) in conjunctiva, 268(89.3%) in lacrimal sac and 272(90.7%) in nasal mucosa. The 77.3% of the overall microorganisms culturedwere gram-positive bacteria, with a predominance of staphylococcus species in conjunctiva and lacrimal sac with Bacillus spp. Group in nasal mucosa. Common association of organism between lacimal sac content and conjunctival sac was 52.3% and between lacrimal sac and nasal mucosa was 33.7% of cases. Conclusion: Antegrade infection is mostly responsible for chronic Dacryocystitis
KEYWORDS: lacrimal sac, chronic dacryocystitis, dacryocystorhinostomy (DCR), conjunctiva, nasal mucosa.
Introduction:
Chronic Dacryocystitis is an inflammatory condition of the lacrimal sac commonly associated with partial and total obstruction of nasolacrimal duct.(1)It is an essential cause of ocular morbidity both in children as well as adults causing chronic tearing,andconjunctival inflammation and infection [2].A unique combination of stasis and moisture in NLDO may create an optimal environment for the growth of lacrimal sac flora. Numerous bacterial species have been implicated in chronic dacryocystitis.(3-4). There are two schools of thoughts regarding the spread of infection leading to nasolacrmial duct obstruction and chronic dacrysocystitis. One being due to infection from conjunctiva (antegrade spread) and other being from the nasal cavity (retrograde spread). Other important sources are infection from paranasal sinuses, allergic rhinitis or deviated nasal septum.Previous studies have suggested that flora of sac and ipsilateral nostril are identical in half of the cases of the chronic dacryocystitis. [5]Accurate identification of the pathogens responsible for chronic dacryocystitis is critical for the selection of appropriate antibiotic agents.[6] Knowledge of the source of infection can significantly contribute in the search of etiology as well as toward the choice of antibiotic. This information can further indentify the source of infection at an early stage thus increasing the possibility of early prevention of the disease. So, this study aims to identify the route and spread of infection to determine whether the source of infection is in conjunctiva or nose.
PURPOSE:
In this study, we aim to indentify the most common route of spread of infection in cases of chronic Dacrysocystitis along with the spectrum of bacteriology.
MATERIALS AND METHODS :
A prospective analysis of microbiological and clinical data of 300 eyes of 260 patients had undergone external dacryocystorhinostomy for chronic dacryocystitis between January 2012 and June 2015 at a tertiary eye care hospital of North East India. There were 186 (62%) females and 114 (38%) males in the age range of 18 to 70 years (mean age 44.2 years). Patients who had a history of acute attack of dacryocystitis and any previous lacrimal sac surgery were excluded from our study. The patients were labelled as chronic dacryocystitis on the basis of history, routine ophthalmic examination by slit lamp, with special attention to the presence of discharge and epiphora confirmed by syringing of the lacrimal drainage system. The materials were collected with sterile cotton tip applicators and sent for culture to the microbiology laboratory. The specimenswereprocessedwithin10–15minutes of their collection. Cultures and smears for the detection of bacterial agents were carried out on the specimens.ENT evaluation in each case was done by the surgeon with the help of the nasal endoscope.
Method of Specimen collection: Three specimens obtained.
First one from the anatomical site of the opening of NLD, at the inferior meatus of the nose of the effected side under endoscopic visualization. The second from the involved side of the conjunctiva and third one from the lacrimal sac under operating microscope during making of the sac flap for external DCR.
The materials were collected with sterile cotton tip applicator and send for culture to microbiology laboratory. The specimens were processed within 10-15 minutes of their collection.
Results :A total of 900 samples of 300 patients with a clinical diagnosis of chronic dacryocystitis were analyzed. Growths were observed in 228(76%) in conjunctiva, 268(89.3%) in lacrimal sac and 272(90.7%) in nasal mucosa.
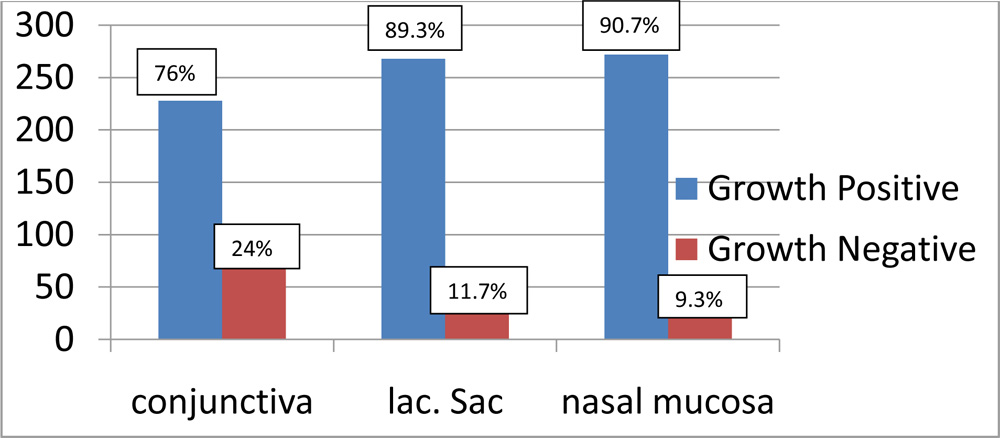
Growths were observed in 228(76%) in conjunctiva, 268(89.3%) in lacrimal sac and 272(90.7%) in nasal mucosa. The 77.3% of the overall microorganisms cultured were gram-positive bacteria, with a predominance of staphylococcus species in conjunctiva and lacrimal sac with Bacillus spp. Group in nasal mucosa.
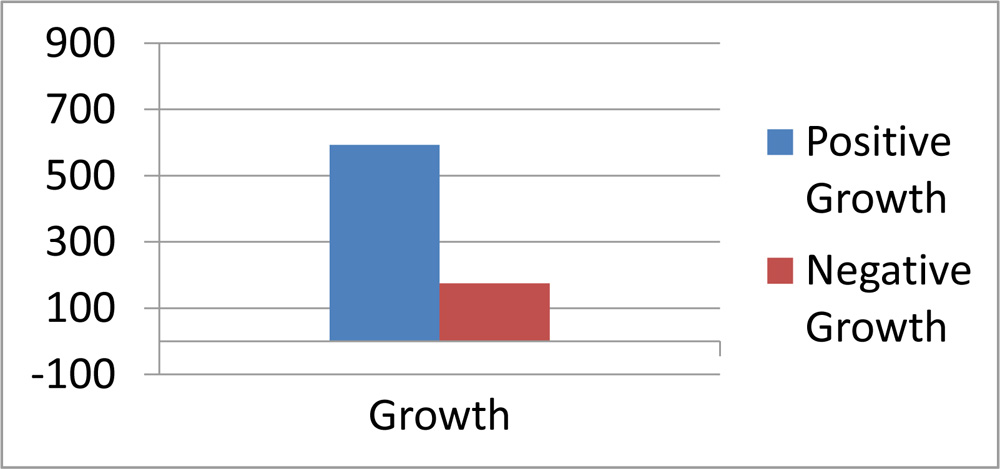
Out of overall 900 samples examined 768(85.3%) were positive and amongst positives, 594(77.3%) samples were having gram-positive bacteria.
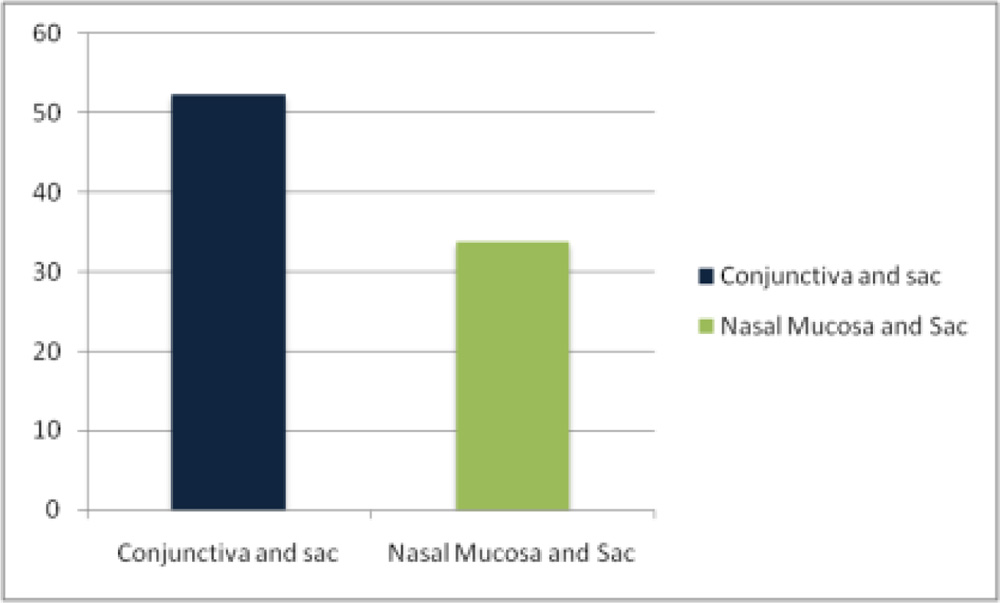
Common association of organism between lacimal sac content and conjunctival sac was 52.3% and between lacrimal sac and nasal mucosa was 33.7% of cases.
Discussion:
Chronic dacryocystitis is an inflammatory condition of the lacrimalsac commonly associated with partial and total obstruction of thenasolacrimal duct, which affects patients of middle age. Severalbacteria have been implicated as causative agents of chronic dacryocystitis [1]. Also, there is a change in the agents responsible for chronic dacryocystitis over the time [2,3]. Knowledge of the microbial organisms responsible for chronic dacryocystitis in a particular geographical area is essential in choosing the appropriate antibiotics [4].Hence we aimed at finding out the bacteria responsible for lacrimal sac infections in the patients visiting this tertiary care hospital and study their antibiogram. In this study comparision was made to isolate ipsilateral nasal mucosa and conjunctival specimens in order to verify the role played by the commensal bacterial flora in the causation of chronic dacryocystitis.
This current study not only contribute the knowledge of organism and sensitivity , also contribute in identifying the source of spread of infection in chronic Dacryocystitis. Statistically significant high association of common organism, between lacrimal sac content and conjunctival sac, indicate that, antegrade infection plays crucial role on chronic Dacryocystitis.
Conclusion:
Antegrade infection is mostly responsible for chronic Dacryocystitis. Knowledge of the source of infection at an early stage, thus increasing the possibility of early prevention of the disease.
References:
1.Das JK, Deka SC, Kuri GC, Bhattacharjee K, Das D, Gogoi K, Orbit 2008;27(4).Bacteriology of Chronic Dacryocystitisin Adult Population of Northeast India
2 Grant GG. Dacryocystitis. J Ophthalmol. 2001;2:1–10.
3.Shun-Shin GA1, Thurairajan G. External dacryocystorhinostomy–an end of an era? BrJOphthalmol. 1997;81(9):716-7.
4.Athanasiov PA, Prabhakaran VC, Mannor G, Woog JJ, Selva D. Transcanalicular approach to adult lacrimal Duct obstruction: a review of instrument and methods. Ophthalmic Surg Lasers Imaging. 2009;40(2):149-59
5.Rajeev N Bale. Dacryocystitis : Bacteriological study and its relation with nasal pathology, IJO 1987:35 (4):178-82
6.Chaudhary M, Bhattarai A, Adhikari SK, Bhatta DR. Bacteriology and antimicrobialsusceptibility of adult chronic dacryocystitis. Nepal J Ophthalmol. 2010;2(2):105-13.