Dr. Narayan S Alane, A18879, Dr. Namra A. Shah, Dr. Shreya Shah, Dr.Pooja Kalbande
Canalicular lacerations are a common injury of the canalicular system. The key step during surgery for the treatment of canalicular laceration is to identify the site of trauma to the canaliculi. On the basis of the canalicular anatomy and microscopic magnification, locating the damaged end of the canaliculi has become simpler.To ensure the normal function of the injured canaliculi after healing, the placement of a silicone tube in the canalicular system has been recommended as a surgical stent during the healing process.The temporary stent intubation could prevent canalicular obstruction during recovery. The advantage of silicone intubation is that it can restore a normal anatomical pathway rather than creating a bypass. Different surgical procedures, such as the pigtail probe, have been introduced to intubate the silicone tube into the canalicular system to repair canalicular lacerations. However, these procedures are regarded as having some limitations and disadvantages. Accordingly, more effective and less invasive methods of silicone tube insertion for the treatment of canalicular lacerations are needed.
Aim:To analyse the pattern of Canalicular lacerations with lid tear, clinical profile & surgical modalities in a tribal population.
Methods:
We retrieved data of patients reporting in oculoplasty department for lid laceration with canalicular involvement. Retrospective epidemiologic data with surgical modalities of repair from hospital data base was tested on standard pretested format & statistical analyses was done.
Results:
The pie diagram below shows sex wise distribution of the cohort
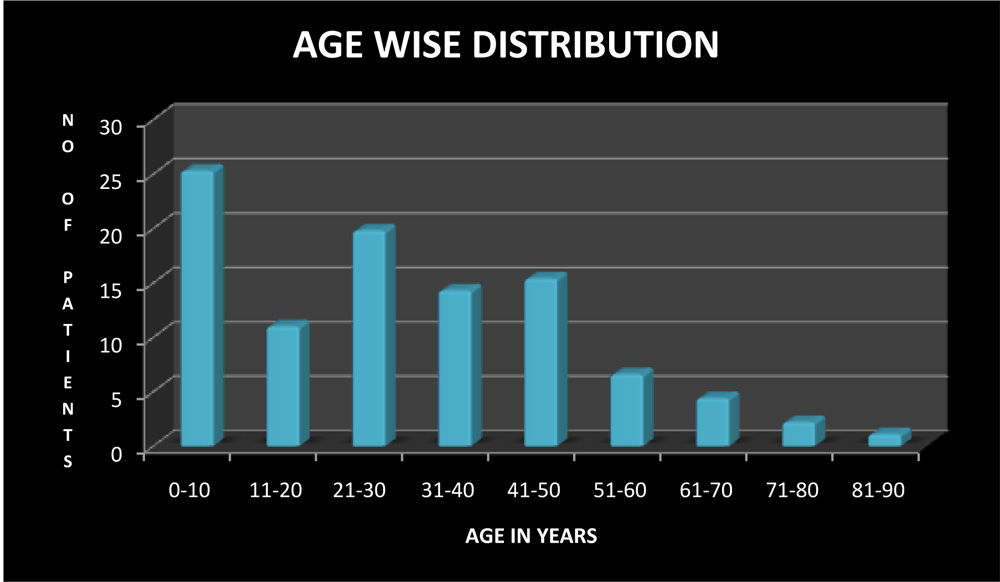
The mean age at presentation was 11.5 years.
The table below depicts the involved eye
The graph shows gender wise distribution in various age groups
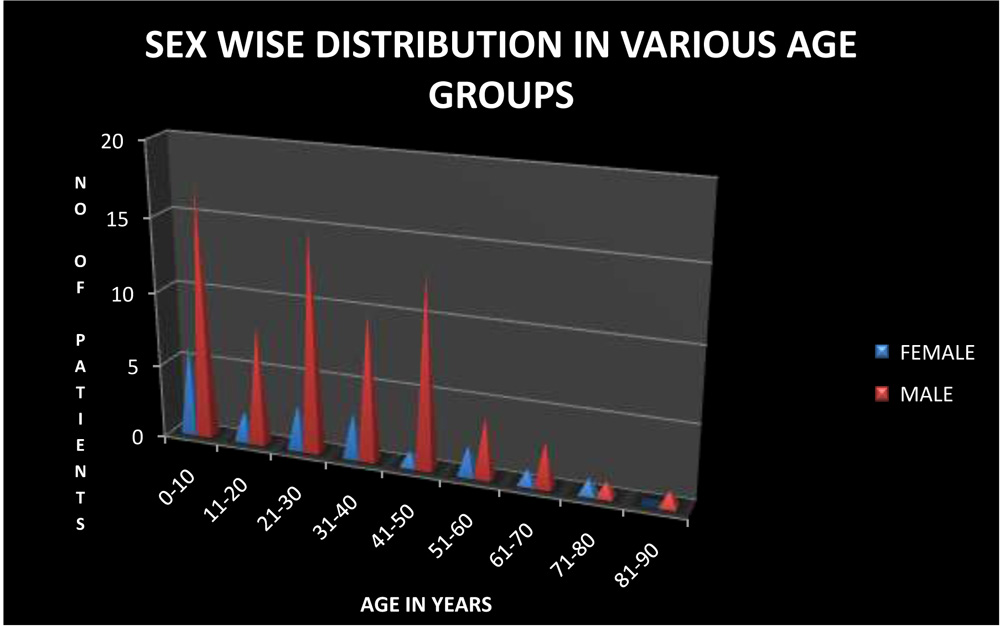
This shows that male population is affected more
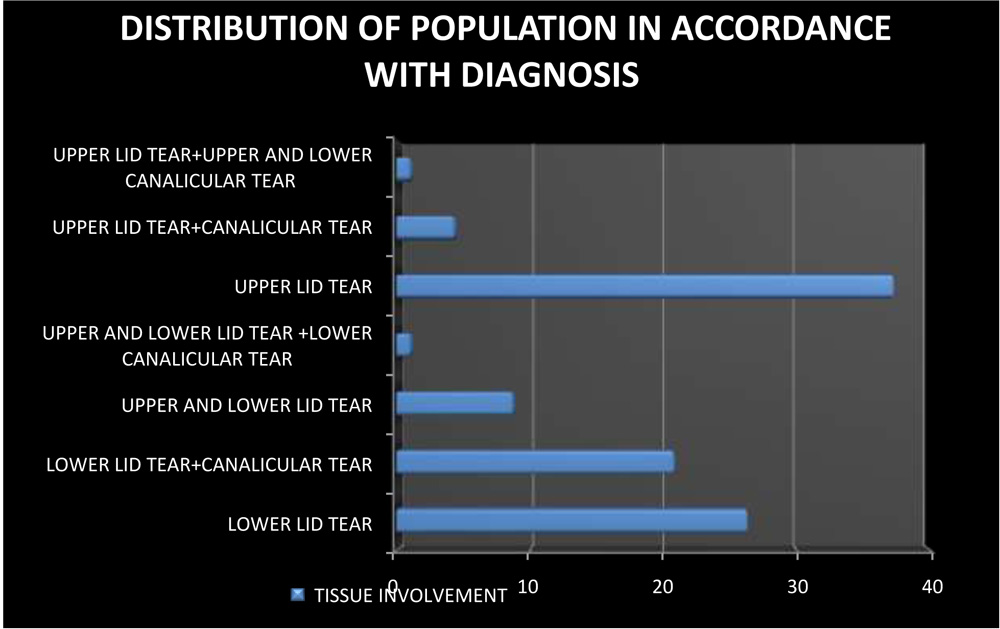
Total 91 patients underwent lid laceration repair. 24 patients had Lower lid tear , 19 patients had Lower lid tear+canalicular tear ,8 patients had Upper and lower lid tear ,1 patient had Upper and Lower lid tear +Lower canaliculi ,34 patients had only Upper lid tear 34, 4 patients had Upper lid tear+ canaliculi tear ,1 patient had Upper lid tear+upper and lower canaliculi tear .
The chart below shows the various cause of injury
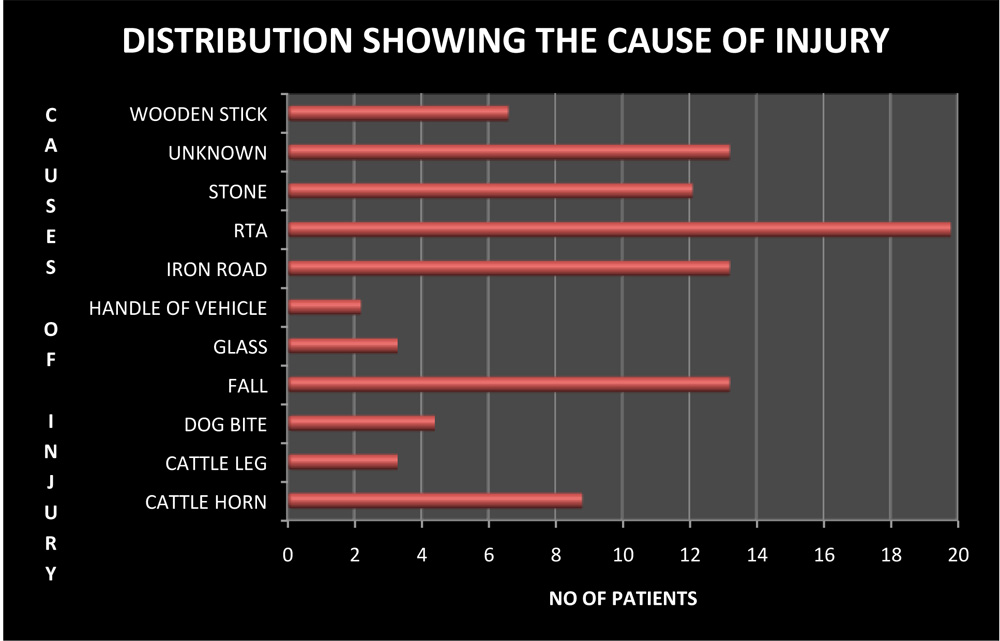
Above graph shows the most common cause of canalicular laceration is Road traffic accidents(20%),followed by fall(13%).
The table below shows the various surgeries performed in cases of lid injuries
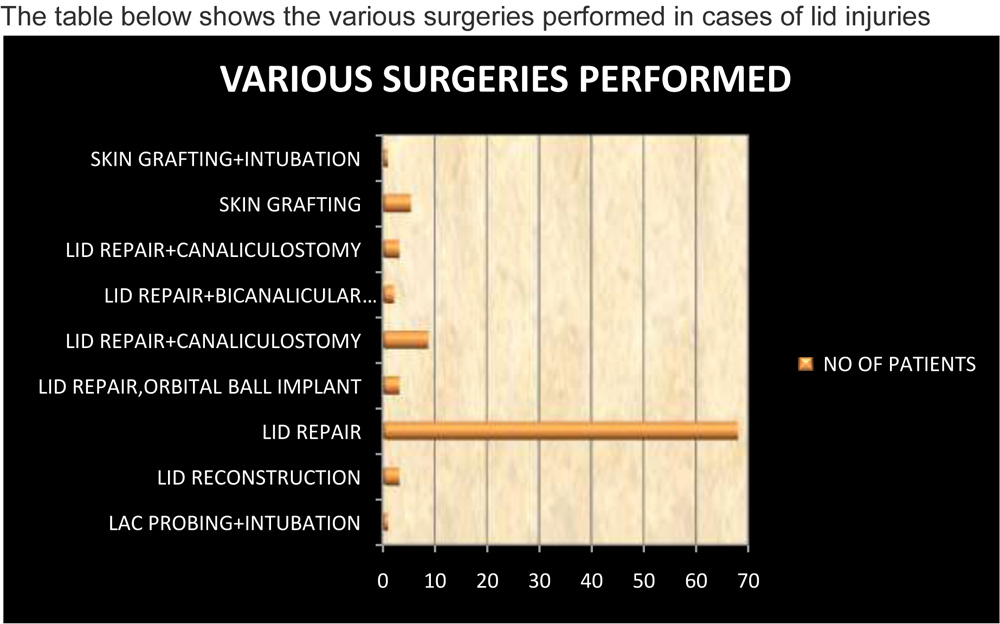
68 % had undergone lid repair,9% had lid with canalicular repair. 4.4% has gone for intubation.3.3 % has bi-canalicular repair with intubation OU., 1.1 % had canalicular repair, skin grafting with intubation.
Discussion-
1Lacrimal system injuries represent a significant part of ocular emergencies and mainly affect males of various ages including very young children. The most frequent presentations are canalicular laceration with a palpebral wound medial to the lacrimal punctum. The inferior canaliculus is the most commonly affected but bilateral injuries or injuries affecting both canaliculi can occur. The main causes are dog bites in children, scuffles in young adults and falls in elderlies. Other lacrimal tract injuries involving the lacrimal sac or the nasolacrimal duct are rare, commonly associated with blunt craniofacial trauma or iatrogenic after some surgical procedures.
2 Pediatric canalicular lacerations are most common in young boys and dog bites are the most common etiology.
3 In lacrimal system lacerations the canaliculi are involved in 70% of cases and the lacrimal sac and/or nasolacrimal duct in 30%. Lacrimal system lacerations can be the result of sharp or blunt trauma. Nasolacrimal ducts may become obstructed by indirect trauma as an aftereffect of naso-orbital fractures. The epidemiology, main principles of surgical repair of canaliculi and of lacrimal sacs and/or nasolacrimal ducts, special techniques of surgical reconstruction and approximate success rates are reviewed with respect to the outcome of our patient collective compared to the literature. Canalicular and lacrimal sac lacerations need urgent primary microsurgical repair with silicone intubation and paying special attention to the medial nasal canthus. In cases of traumatic nasolacrimal duct obstruction as an aftereffect of mid-facial fractures, a secondary reconstruction should be planned.
4 Direct, indirect, or diffuse forces may injure canaliculi but direct penetrating injuries were more common than avulsive injuries. More serious injuries (orbital fractures, globe rupture, other body injuries, and head trauma) were more commonly seen when diffuse trauma was involved.
5 Success rate of canalicular laceration with silicon intubation was found to be 80%
6 Success rate of 20G silicon rod as monocanalicular intubation was found to be 70%.
Conclusion:
Lid repair with intubation appears to be successful in the management of canalicular injury.
References
1)[Lacrimal traumatology]. Ducasse A,arndt C
Jfr ophthalmol 2016 Feb;39(2):213-8
2)Pediatric canalicular lacerations: epidemiology and variables affecting repair success. JPediatr ophthalmol strabismus 2014 Jul 1;51(4):242-8
[Lacrimal system lacerations and their surgical repair].
Struck HG
3)Ophthalomoge 2009 Mar;106(3):223-8.
4)Pathogenesis of canalicular lacerations.
Ophthal plast reconst surg2008 Sep-Oct;24(5):394-8.
5)Chatterjee S, Rath S, Roy A, Shrestha E. 20G silicone rod as monocanalicular stent in repair of canalicular lacerations: Experience from a tertiary eye care centre. Indian J Ophthalmol 2013;61:585-6
6) Tabatabaei S.Z, Sarvarian A, Kasaei A . Repair of canalicular laceration with silicone intubations. . Iranian Journal Of Ophthalmology 2004; 16(2): 41-49.

