Dr. Rushita R Kamdar, R15509, Dr.
Jagadeesh Kumar Reddy K, Dr. Neeraj Shah, Dr.
K S Siddharthan
Abstract:
Purpose: To evaluate distance and near visual outcomes and photic phenomena of a hybrid optic multifocal IOL.
Methods: A prospective, non-randomized clinical case series was performed wherein 40 eyes of 36 patients with senile cataract were implanted with hybrid optic IOL, an IOL with refractive optic for distance and a single, small, central diffractive optic element for near, after phacoemulsification. Visual acuity, Spectacle independence, presence of photic phenomena and patient satisfaction were assessed post-surgery.
Results: 40 eyes had BCVA for distance 20/20 and near vision with distance correction N6. UCVA of 36 patients is 20/30 or better, 4 patients is 20/40. 40 patients had UCVA for near N8 or better and 34 had UCVA for near N6. All the patients were satisfied with their subjective visual quality and only one of them reported photic phenomena on questioning. 36 patients achieved spectacle independence.
Conclusion: This IOL successfully restores both near and distance vision without any photic phenomenon. It eliminates the visual disturbances associated with diffractive optic design IOL for distance vision.
Introduction
Modern cataract surgery with an intraocular lens (IOL) has the potential to improve a patient’s acuity and refine the refractive error to a given target. But, presbyopic correction sans spectacles still remains the Holy Grail post cataract surgery. By design, monofocal IOLs are limited in range, typically achieving distance, intermediate, or near, but rarely encompassing all distances. The “ideal” IOL would restore the patient’s vision without visual compromises and allow the patient to regain his or her ability to see at all distances.
Since long time, different approaches to IOL design have evolved in an effort to address the impact of presbyopia, and new strategies and technologies will continue to appear. The multifocal IOLs are designed with refractive and/or diffractive optical properties, which focus light on multiple foci and allow the patient to see both near and distant objects.[1-11] Since the light energy is distributed between more than one image and some energy is lost to useless foci, each primary image produced by a multifocal IOL is thereby fainter and defocused at any given pupil aperture, compared to monofocal or accommodating IOLs that do not split up light in this manner.[1,2] Diffractive multifocal IOLs provide good levels of distance and near visual acuity independent of pupil diameter, but they are associated with reduced efficiency at intermediate distance and decreased contrast sensitivity for distance and significant dysphotopsia in the form of glare and haloes.[2]
The fact remains that neither monovision, nor multifocal IOLs nor accommodating IOLs offer a suitable solution.We describe our initial results with a hybrid intraocular lens which provides optimum vision at two focal planes – distance and near both without the occurrence disturbing photic phenomena.
Materials and MethodsL
FORMAT HAS TO BE CORRECTED) Ethics Committee approval was obtained.Informed consentwasobtainedfromallpatientsenrolledbetweenFeb2015tillJan2016.Thestudycohortcomprisedpresbyopicametropicpatientsintheagegroup40-65yearswithcataract.40eyesof36patients were enrolled in this study. TheyunderwentstandardphacoemulsificationwithimplantationofthisHybridIntraocularlens with 3.5 D near addition. Four patients had bilateral implantation of the lens.Patientswereenrolledaftercarefulselectionandscreening.Exclusioncriteriawereahistoryofglaucoma,retinaldetachment,cornealdisease,cornealsurgery,ocularinflammation,neuroophthalmicdisease,maculardegenerationorretinopathy,keratometriccylindergreaterthan1.00diopter(D)andsenilemioticpupils,patientswithtraumaticmydriasisoririscoloboma.Allpatientshadapreoperativeexaminationthatincludedautorefraction, tonometry, uncorrected and corrected distancevisualacuity(UDVA, CDVA), nearvisualacuity, biometry(IOLMaster 500,CarlZeissMeditecAG),subjectiveandcycloplegicrefractions,slit-lampevaluationanddilatedfundusevaluation.VisualacuitywasmeasuredatdistanceandnearvisionwithaSnellenvisualacuitychartandconvertedtologMARscores. Axiallength(AL),anteriorchamberdepth (ACD),andkeratometry valuesfromtheIOLMasterwereusedforIOL powercalculation.Alleyesweretargetedforemmetropia.UDVAandCDVA,uncorrectednearvisualacuityanddistance-correctednearvisualacuity(UNVAandCNVA),wereevaluatedat1week, 1month,6monthsand10monthslater.Spectacle independence for the operated eye and patient satisfaction was also analyzed.
Intraocularlens-TheIOLisasinglepiecehydrophobicacrylicfoldable13mmlenswithanopticof6mm.Ithasasymmetricbiconvexdesignwithananteriorasphericprofile.The IOL has an unique design wherein its refractiveopticharboursacentralsmallDiffractiveOpticelement(DOE)segmentof+3.5dioptresadd.Thiswouldtranslatetoanaddof2.57Datthespectacleplane.
Surgical Technique -The surgeries were performed by a singlesurgeon.The pupils were dilated with Tropicamide+PhenylephrineandCyclopentolate.Proparacaine (0.5%) and Lignocainejelly(4%)wasapplied.Lensextractionwasperformedusingastandardphacoemulsificationtechniquethrougha2.8mmincision.Allincisionsweremadeonthesteepestcornealmeridiantoneutralizecornealastigmatism.Afterphacoemulsification,the hybridfoldableIntraocularlenswasinsertedthrough a 2.8mm corneal incision using the injectorinto the capsular bag ensuring adequate centration.Postoperatively,patientswereaskedtoinstillGatifloxacin(0.3%)withLoteprednoletabonate (0.5%)taperedoveramonthalongwithNepafenac(0.03%) for60days.
Results
The mean follow up of these patients was recorded as 12.25 months (8-18 months).The mean patient age was calculated to be 55 years (46-64 years).16 were males and 24 were females. Postoperatively, all patients had a well centred IOL within the capsular bag with a normal Anterior Chamber. Figure 1& 2 depicts post-operative anterior segment photograph of a patient with this IOL.
Figure 1:
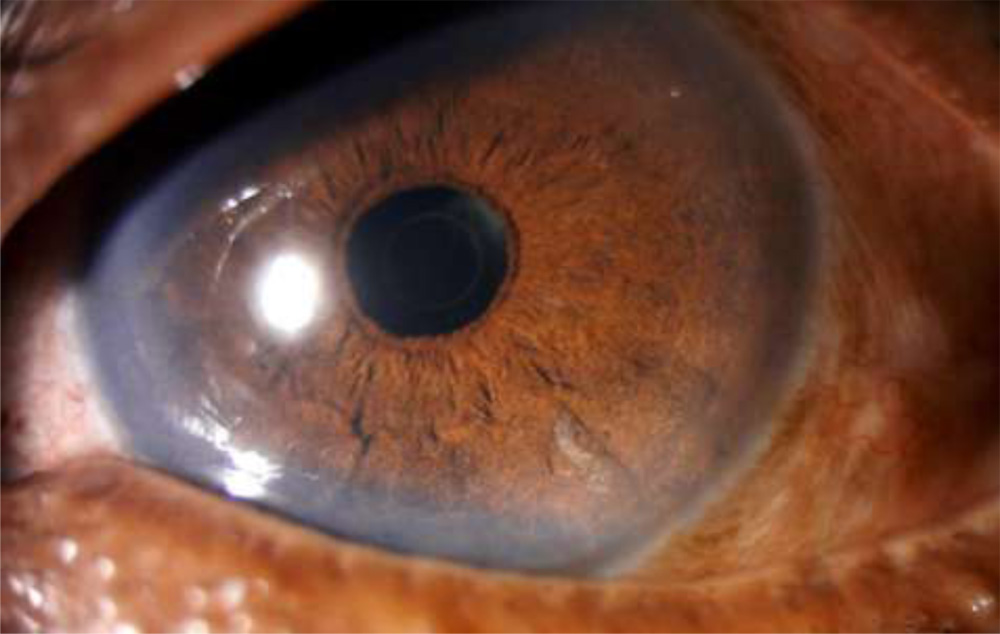
Figure 2 :Post dilatation:

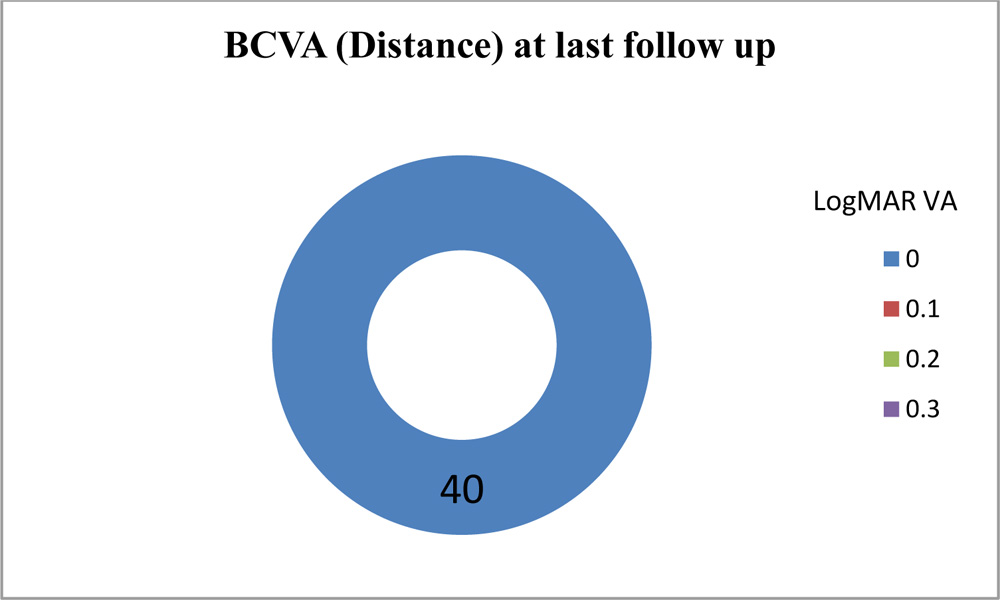
All 40eyes(100%) hadBCVAfordistance20/20andnearvisionwithdistancecorrectionN6 which was well maintained till their last follow up.(Figure 3)
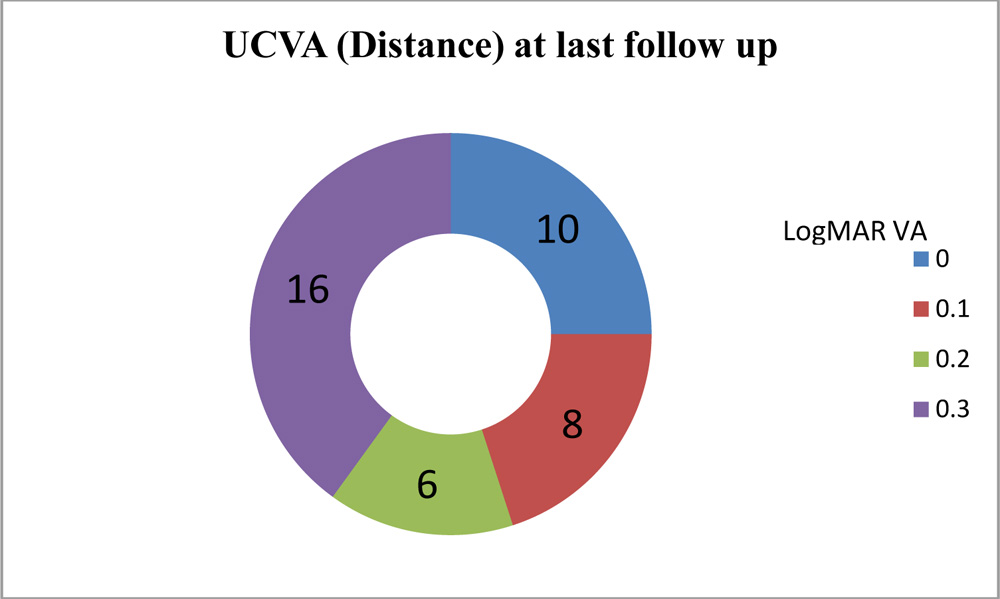
UCVA of 36 eyes (90%) is 20/30 or better, and remaining 4 eyes patients is 20/40. (Figure 4)
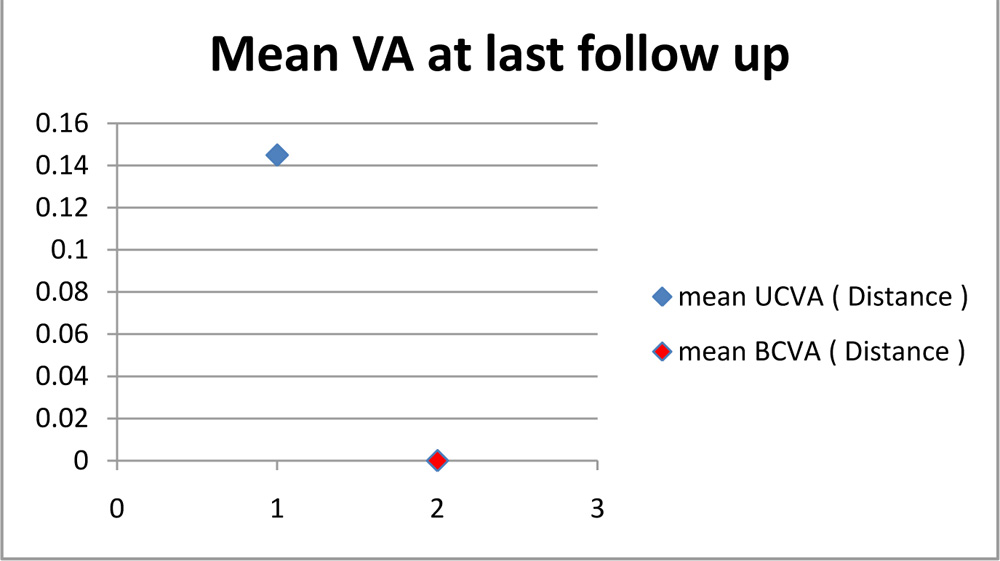
Mean UCVA for distance is 0.145. Mean BCVA for distance is 0.0 (Figure 5)
Figure 5
40patients(100%)hadUCVAfornearN8orbetterand34 (85%)hadUCVAfornearN6.(Figure 6)
Figure 6
Allthepatientswerehighlysatisfiedwiththeirsubjectivevisualqualityandonlyonereportedanyphoticphenomenaonquestioning (p=0.025).
36patientsachievedspectacleindependence intheoperated eye. All four patients with bilateral implantation of this new design IOL had excellent spectacle free vision for both distance and near.
Discussion
In our study, eyes with the hybrid lens implantation had a mean UCVA for distance 0.145 and mean BCVA for distance 0.0.In other studies implanted with the ReSTOR IOL, 99.3% achieved 20/40 or better visual acuity. [11] (100%) had UCVA for near N8 or better and 34 (85%) had UCVA for near N6. In comparison, binocular uncorrected near visual acuity results demonstrated that 96.7% of the ReSTOR patients achieved 20/40 or better, with 40% having 20/20 or better vision. [11]
The excellent visual acuity at two focal planes- distance and near is provided by its novel design.TheIOLisasinglepiecehydrophobicacrylicfoldable13mmlenswithanopticof6mm.Ithasasymmetricbiconvexdesignwithananteriorasphericprofile.ThisrefractiveIOL’sopticharborsacentralsmallDiffractiveOpticelement(DOE)segmentof+3.5dioptersadd.Thiswouldtranslatetoanaddof2.50Datthespectacleplane.Thecentralsegmentfocusesraysfromthenearobjectontotheretina.Thecentralsmallsegmentprovidesincreaseddepthoffocusduetoitspinholesimulatingeffect.Theperipheralareaoftherefractiveopticdirectslighttoadistancefocalpointandisdedicatedtodistancevision.However,duringdistantworktheeffectofthecentralsegmentisnegligibleduetoitssmallsizewhichinturnwouldleadtoasuperimpositionofaninsignificantblurofthenearimageonthedistantimage.[13] The human brain must adapt to this process of simultaneous imaging.[14]
Refractive multifocal intraocular lenses are pupil dependent, incorporating different refractive zones to create focal points at varying distances.[14] DiffractiveIOLs, though pupil dependant,achievemultifocalitybycreationofmultipleringstepsofvariableheightsontheoptic.[14]Thisdesignhowevercreatesaperceptionofglareorhaloesaroundthedistantimageduetosuperimpositionofnearimageblur.ThedesignofthishybridIOLpotentiallyavoidsthesecompromisestoofferabetterqualityofvision.
Thisnovel lensisdependent onpupilsize, to its advantage.Inastateofambientlightconditionswhentheusualpupilsizewouldbe3.5–4mm,majorityofthelightenergyisfocusedfordistancewithonly 9%focusedfornear.Atnightinastateofpupillarydilatation,thequantaofenergydirectedfordistanceproportionatelyrisesto80%withameagre4%energypassingthroughthecentralDOEpreservinggoodcontrastsensitivityandminimizingtheincidenceofglare,haloes,ghostingofimages.ThisisincontrasttoallDiffractiveMultifocalIOL’swherea significantly large percentageofthelightenergywouldbefocusedforneardistanceresultinginintolerableglareandhaloes.[1,2] Duringnearwork,thepupilsizereducesresultinginproportionateincreaseintheenergyfocusedthroughthecentralsmallDOE(nearly 40%)resultinginoptimumnearvisualacuity.
Althoughtheoreticallyaperfectlyclearandin-focusretinalimageispresentonlywhenitispreciselyopticallyconjugatewiththeretinaitself,aslightlydefocusedimagewillalsobeinterpretedinthiswaybythebrainaslongasitispositionedwithintheopticalextentofthedepth-of-focus.Aslongasatargetremainswithinthedepth-of-fieldinobjectspace,itsretinalimagewilllikewiseremainwithinthedepth-of-focusinimagespace,andhenceclarityofthetargetwillbeperceived.[13]SincethisIOLutilizestheprinciplesofrefraction,diffractionandextendeddepthoffocus,itwouldbeapttocallitahybrid iol.
Weutilizedaself-madequestionnaire,inquiringtheincidenceofglare,haloes,difficultyinnightdriving,satisfactionwithvisualqualityandiftheywouldsuggestthisIOLimplantationtootherpatients.Onlyonepatientcomplainedofdifficultyofdrivingatnight.AllpatientsweresatisfiedwiththisIOLandwerewillingtosuggesttheimplantationofthislenstotheiracquaintancestoo.
Theoretically,feweropticalsideeffectsofthenewIOLshouldbeexpectedbecausetherearenoringsegmentsintheopticforrefractionordiffractionandtheembeddednearsegmentreflectsonlyaminimalquantaofenergy.ThepresenceofonlyasingletransitionzonebetweentherefractiveopticandcentralDOEwilldefinitelyreducethesourceofscatteringandaberrations,minimizeglareandhaloesandimprovecontrastsensitivity.
Though our initial results with the new design IOL have been extremely gratifying , we need further follow up with a larger sample size. Another limitation would be we did not have a control group to determine whether multifocal IOL implantation is associated with better satisfaction/visual function compared with monofocal IOLs. Also, we focused only on self-reported satisfaction and visual function. Future studies in our population are needed to
examine the effects of multifocal IOLs on both distance, intermediate and near visual acuity and contrast sensitivity.
Conclusion:
This hybrid IOL successfully restores both near and distance vision without any photic phenomenon. It eliminates the visual disturbances associated with diffractive optic design IOL for distance vision. With careful selection of cases and preoperative patient education, the hybrid IOL may become an important tool in the present day cataract surgeon’s armamentatarium. However, long term studies and a large sample size is needed to validate this product conclusively.
References
- Davison JA, Simpson MJ. History and development of the apodized diffractive intraocular lens. J Cataract Refract Surg2006;32:849-858.
- D. Allen, R. L. Burton, S. K.Webber et al., Comparison ofa diffractive bifocal and a monofocal intraocular lens, Journalof Cataract and Refractive Surgery, vol. 22, no. 4, pp. 446–451,1996.
- Vingolo EM, Grenga P, Iacobelli L, Grenga R. Visual acuity and contrast sensitivity: AcrySofReSTORapodized diffractive versus SA60AT monofocal intraocular lenses. J Cataract RefractSurg2007;33:1244-1247.
- Pepose JS. Maximizing satisfaction with presbyopia-correcting intraocular lenses: the missing links. Am J Ophthalmol2008;146:641-648.
- Pepose JS, Altmann GE. Comparing pupil-dependent image quality across presbyopia-correcting intraocular lenses. J Cataract Refract Surg2010;36:1060-1061.
- Castillo-Gómez A, Carmona-González D, Martinez-de-la Casa JM, Palamino-Bautista C, García-Feijoo J. Evaluation of image quality after implantation of 2 diffractive multifocal intraocular lens models. J Cataract Refract Surg2009;35:1244-1250.
- Ortiz D, Alío JL, Bernabéu G, Pongo V. Optical performance of monofocal and multifocal intraocular lenses in the human eye. J Cataract Refract Surg2008;34:7762.
- Martinez Palmer A, Gomez Faiña P, EspañaAlbelda A, Comas Serrano M, NahraSaad D, CastillaCéspedes M. Visual function with bilateral implantation of monofocal and multifocal intraocular lenses: a prospective, randomized, controlled clinical trial. J Refract Surg2008;24:257-264.
- Montés-Micó R, España E, Bueno I, Chapman WN, Menezo JL. Visual performance with multifocal intraocular lenses; mesopic contrast sensitivity under distance and near conditions. Ophthalmology 2004;111:85-96.
- Artigas JM, Menezo JL, Peris C, Felipe A, Díaz-Llopis M. Image quality with multifocal intraocular lenses and the effect of pupil size. Comparison of refractive and hybrid refractive-diffractive designs. J Cataract Refract Surg2007;33:2111-2117.
- Weghaupt H, Pieh S,Skorpik C. Visual properties of the foldable Arraymultifocal intraocular lens. J Cataract Refract Surg1996; 22:1313-1317.
- Lane SS,Morris M, Nordan L, Packer M, Tarantino N,R. Bruce Wallace III. Multifocal Intraocular Lenses. OphthalmolClin N Am 19 (2006) 89 – 105.
- Depth-of-Focus of the Human Eye: Theoryand Clinical Implications. Wang B,Ciuffreda KJ .Survey of Ophthalmology 2006 ;vol 51;1:76-86.
- Multifocal Intraocular lenses –the art and the practice . Essentials of Ophthalmology . Edited by Alio J, Pikkel J. Springer Publications.