Dr. Isha Khaitan, K18218
Dr. Thakkar Hansa Harshadbhai
Presenting Author: Dr. IshaKhaitan
Co-Author: Dr. Hansa H Thakkar
Institution: M & J Western Regional Institute Of Ophthalmology, Ahmedabad.
Email: ishakhaitan@yahoo.in
Phone No: 9687002658
Anterior Segment Imaging in Pseudophakic Corneal Oedema
Abstract
Purpose:
To evaluate role of Ultrasound Biomicroscopy( UBM )and Anterior Segment Optical Coherence Tomography ( AS OCT ) in psuedophakic corneal oedema.
Method:
Thirty pseudophakic patients with corneal oedema were enrolled in prospective study. After complete ophthalmic examination, patients were subjected to UBM and AS-OCT. Patients with trauma and pre-existing ocular disease were excluded.
Results
Out of 30 patients 8 were males and 22 females. Descemet’s tear was observed in 5 on SLE, 8 on ASOCT and 11 on UBM. Anterior synechiae was detected in 1 on SLE, 4 on AS-OCT and 7 on UBM. IOL malposition was seen in 8 on SLE and 18 on UBM. IOL status could not be assessed in 15 patients on ASOCT. Iris IOL clearance and Haptic were seen only by UBM.
Conclusion:
AS-OCT provides good resolution of epithelial lesions. UBM has distinct advantage over OCT for visualizing angle structures, ciliary body, optic and haptic of IOL. It clarifies the mechanism of edema and hence guides further management
Keywords:UBM, ASOCT, Corneal oedema, IOL malposition
Introduction:
Recent innovations in instruments and surgical techniques have led to improvement in visual outcome following cataract surgery.[1]Nevertheless,postoperative corneal oedema remains a common cause of visual deterioration following cataract surgery.
Factors that pre-dispose to corneal oedema following cataract surgery include the following: intraoperative mechanical endothelial trauma, prior endothelial disease or cell loss, excessive postoperative inflammation and prolong postop elevation of IOP. [2]
Corneal oedema makes the clinical examination difficult. In the absence of any evidentcause,it becomes difficult to treat such cases. Patients are therefore usually offered only symptomatic treatment. In such situations UBM and ASOCT have a significant role in altering the diagnosis and management.
In this study we aimed at assessing patients with corneal oedema after cataract surgery using high resolution anterior segment imaging. The results of the study enabled us to understandthe cause of underlying corneal oedema and hence precise management was possible.
Materials and Methods:
30 patients with corneal oedema after cataract extraction with IOL implantation were enrolled in our prospective study done between December 2014 to May 2016.Patients with traumatic cataract, pre-existing ocular diseases & postoperative endophthalmitis were excluded from the study. Surgeries were performed by surgeons at various eye clinics. The study was performed with informed consent and followed the guidelines of the ethics committee of the institute.
All the patients were subjected to basic history taking, visual acuity testing, through clinical and slit lamp examination, fundus and B-scan imaging. After a through work-up patientswere sent for ASOCT and UBM imaging performed by the same technician and ophthalmologist respectively.
Patients were imaged with ZEISS VisanteOCT Model 1000. The Visante OCT is based on low coherence interferometry using a 1310 nm infrared light with an axial resolution of 18 μm. The ASOCT assesses the thickness of the cornea along its entire surface. Analogous to an ultrasound B‐scan, Visante OCT acquires multiple A‐scans and aligns them to construct two dimensional images.[3]
UBM at our institute (OTI 2000) uses high frequency ultrasonography (50 MHz) and requires an eye bath with supine position of the patient. After anaesthetizing the ocular surface and introduction of water bath cross-sectional images of the anterior segment were obtained. Patients were examined indetail for thickening of cornea, depth of AC, angle anatomy, signs of inflammation and IOL position and iris-IOL clearance.
Results:
Out of 30 patients 8(27%) were males and 22(73%) females, age ranged from 35-85 years (mean 63.85). 11(37%) patients had right eye involvement whereas 19(63%) had left eye involvement.
Image analysis revealed descemet’s tear in 5(17%) on SLE, 8(27%) on ASOCT and 11(37%) on UBM [Figure 1]. Anterior synechiae were detected in 1(3%) on SLE, 4 (13%) on ASOCT and 7 (23%) on UBM respectively.Uveitis along with pars planitis was detected in 5(17%) by SLE and UBM but couldn’t be assessed by ASOCT. Thick Ciliary body, cyclodialysis cleftand angle recession were seen only on UBM[Figure 2].
IOL malposition was the commonest cause of corneal oedema in our study.It was seen in 8(27%) on SLE and 18(60%) on UBM. IOL status could not be assessed in 15(50%) and optic was only faintly seen in 15 (50%) on ASOCT [Figure 3].
Among malpositionedIOL, ACIOL was found in 4 (13%) on SLE and 5(17%) on UBM, Tilted IOL 3 (10%) on SLE and 12 (40%) on UBM and IOL in sulcus in 1 (3%) on both SLE and UBM[Figure 4]. Haptic of 1(3%) IOL was seen touching the sulcus, 2 (7%) ciliary body and 1(3%) angle structures on UBM. 8 (27%) patients showed poor iris IOL clearance on UBM. In 1(3%) patient ASOCT underestimated corneal thickness.
The results are shown in Table 1.
Discussion:
Chronic corneal oedema is most commonly related to elevated IOP, intraocular inflammation or endothelial dysfunction.[4]Corneal oedema due to inadequate endothelial pump function is one of the most common complications of cataract surgery.
Descemet’s membrane detachment (DMD) following cataract surgery can present with severe corneal oedema and marked reduction in visual acuity.DMD can be easily overlooked or misdiagnosed. In our study DMD was detected in 37% patients on UBM, which was missed on clinical examination.According to Dr. Ram et al“DMD should be suspected in patients showing unexpected corneal edema postoperatively who have undergone uneventful phacoemulsification and be treated in a timely manner”[5]
Increased IOP following cataract surgery is due to inflammatory cells, block in trabecular mesh work, iris bombe or PAS [Figure5]. Inflammation especiallyiritis and uveitis can profoundly affect endothelial function.[6]Haptic of malpositioned IOL can irritate uveal tissue leading to chronic inflammation.
Pavlin et al were the first to describe UBM images of cornea.[7]Huang et al[8]first described optical coherence tomography of the eye in 1991, and Izatt et al described ASOCT using the same wavelength of light as in retinal OCT i.e. 830nm.[9]Recent advances in OCT technology have allowed for high-speed scanning of cornea and anterior segment.[10]
In cases of dense corneal oedema detachment and re-attachment of descemet’s membrane can be assessed with ASOCT and UBM. Both UBM and ASOCT can be used as a diagnostic tool in uveitis with small pupil. UBM is an excellent tool to delineate exudates and membrane over pars-plana region [Figure6]. In IOL induced uveitis UBM confirms the position of IOL haptic and any structural damage caused by it.
UBM has unique advantage of enabling visualization of structures posterior to iris such as ciliary body, zonules and peripheral lens.However, UBM isa contact method, and requires a highly skilled operator in order to obtain good quality images.
ASOCT produces higher resolution images and can beperformed in immediate post op period. However, asASOCT uses light, it loses accuracy and resolution as stromal oedema or opacification increase. UBM provides the most accurate measurement when there is sign of stromal oedema.[11] In this study OCT underestimated corneal thickness in one patient.
To our knowledge, this is the first study comparing ASOCT and UBM in the evaluation of pseudophakic patients with corneal oedema.
We found this high-resolutionimaging to bevery helpful in diagnosing and managing patients with corneal oedema. Ithelped us to overcome the obvious limitation of clinical and slit lamp examination.
This comparative study gave us the confidence in the reliability of UBM in imaging of pathology posterior to iris. We now routinely use UBM to evaluate patients with persistent post op corneal oedema.
UBM offers better visualization and provides over all better images compared to ASOCT in presence of dense oedema. Introduction of the use of such minimally invasive diagnostic tool can potentially enable an optical biopsy in vivo.[12]
Conclusion:
Both UBM and ASOCT dramatically improves resolution of anterior segment structure by noninvasive means. UBM is the imaging modality of choice in psuedophakic corneal oedema.
It visualizes the anterior segment of eye with images similar to low magnification histological sections.[13]UBM helps to precisely resolve diagnostic dilemma in post op corneal oedema.
The information hence obtained is of immense help in clarifying the root cause of edematous cornea and deciding further management thereby enhancing quality of life in our patient.
References.
1.Do JR, Oh J-H, Chuck RS, Park CY. Transient Corneal Edema is a Predictive Factor for Pseudophakic Cystoid Macular Edema after Uncomplicated Cataract Surgery. Korean Journal of Ophthalmology : KJO. 2015;29(1):14-22. doi:10.3341/kjo.2015.29.1.14.
2.Reddy MK. Complications of cataract surgery. Indian J ophthalmol 1995;43:201-9
3.Leung CK, Yick DW, Kwong YY, et al. Analysis of bleb morphology after trabeculectomy with Visante anterior segment optical coherence tomography.The British Journal of Ophthalmology. 2007;91(3):340-344. doi:10.1136/bjo.2006.100321.
4.Edelhauser HF. The balance between corneal transparency and edema: the Proctor Lecture. Invest Ophthalmol Vis Sci 2006;47:1754-67.
5.Sukhija J,Ram J, Kaushik S, Gupta A. Descemet’s membrane detachment following phacoemulsification.Ophthalmic Surg Lasers Imaging. 2010 Sep-Oct;41(5):512-7. doi: 10.3928/15428877-20100625-02. PMID:20672769
6.Kang HM, Park JW, Chung EJ. A retained lens fragment induced anterior uveitis and corneal edema 15 years after cataract surgery.Korean J Ophthalmol. 2011 Feb. 25(1):60-2.
7.Pavlin CJ, Harasiewicz K, Sherar MD, Foster FS. Clinical use of ultrasound biomicroscopy.1991;98:287–95.
Huang D, Swanson EA, Lin CP, et al. Optical Coherence Tomography.Science (New York, NY). 1991;254(5035):1178-1181.
8.Izatt JA, Hee MR, Swanson EA, et al. Micrometer-Scale Resolution Imaging of the Anterior Eye In Vivo With Optical Coherence Tomography.Arch Ophthalmol.1994;112(12):1584-1589. doi:10.1001/archopht.1994.01090240090031.
9.High-speed Optical Coherence Tomography of Corneal Opacities; Khurana, Rahul N. et al. Ophthalmology , Volume 114 , Issue 7 , 1278 – 1285
10.American Academy of Ophthalmology Cornea/External Disease Panel. Preferred Practice Pattern® Guidelines. Corneal Ectasia. San Francisco, CA: American Academy of Ophthalmology; 2013.
11.C.Kr, h. Th. Ultrasound biomicroscopy as an important diagnostic adjunct in the management of limbal tumors. Ijcrr. 2014; 6(21): 35-40.
12.Ultrasound Bio Microscopy in Evaluation of “Complicated Pseudophakia”. Indian J ophthalmol. 2010; 152-154
Legends:
Table 1:Findings on SLE, ASOCT and UBM in Psuedophakic corneal oedema
Figure 1: Descemet’s detachment on UBM & ASOCT.
Figure 2: UBM showing thick ciliary body.
Figure 3: ACIOL on UBM. IOL status could not be assessed on ASOCT
Figure 4:Sites of malpositioned IOL.
Figure 5(a and b): Iris bombe on UBM and ASOCT
Figure 6:Exudates over pars plana on UBM.
Table 1: Findings on SLE, ASOCT and UBM in psuedophakic corneal oedema
| No. | Observation | SLE | AS-OCT | UBM |
| 1. | Descemet tear | 5 | 8 | 11 |
| 2. | PAS | 1 | 4 | 7 |
| 3. | Iris Bombe | 1 | 2 | 2 |
| 4. | Post Synechiae | 3 | 7 | 9 |
| 5. | Uveitis | 5 | 0 | 5 |
| 6. | Thick CB | 0 | 0 | 1 |
| 7. | Cyclodialysis cleft | 0 | 0 | 1 |
| 8. | AR | 0 | 0 | 1 |
| 9. | Superior iridodialysis | 1 | 1 | 1 |
| 10. | Iris IOL clearance (Poor) | 0 | 0 | 8 |
| 11. | Optic capture | 3 | 3 | 9 |
| 12. | IOL Malposition | 8 | 15(faint) | 18 |
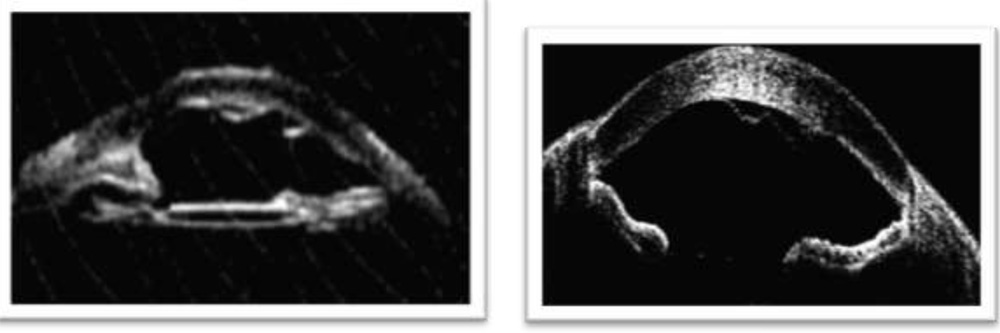
Figure 1: Descemet’s detachment on UBM & ASOCT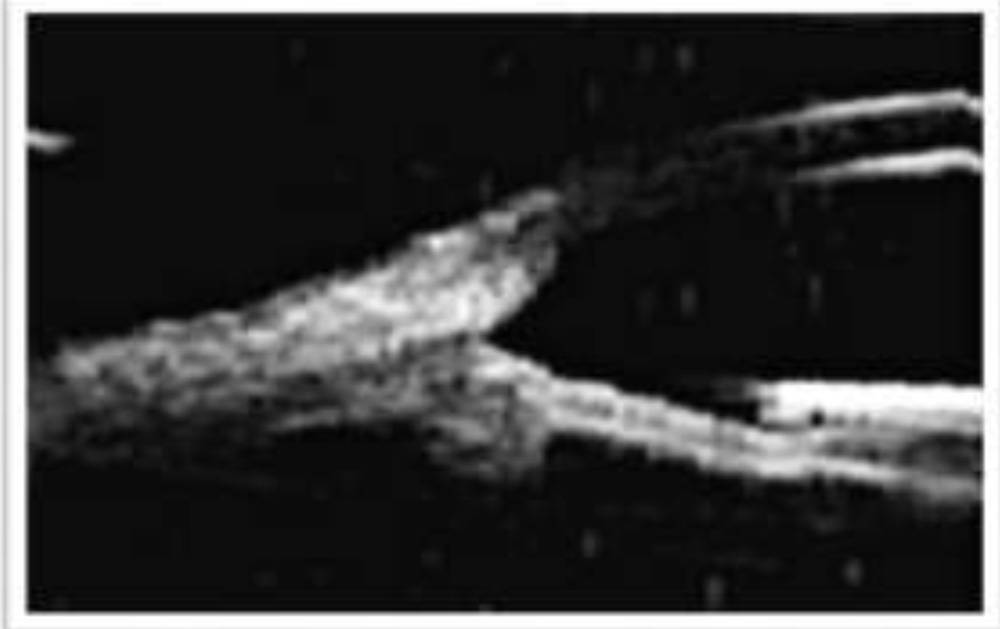
Figure 2: UBM showing thick ciliary body.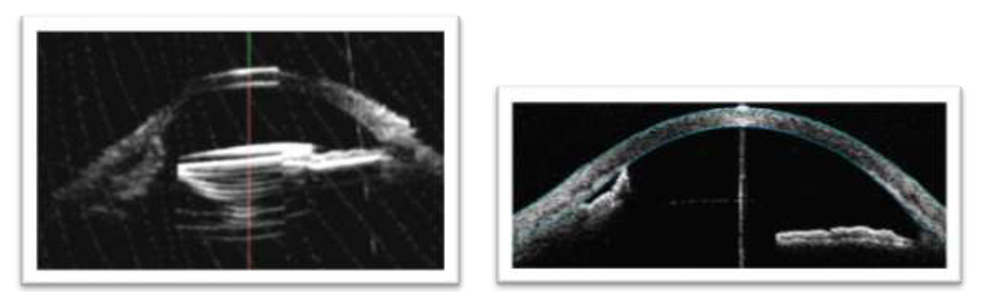
Figure 3: ACIOL on UBM. IOL status could not be assessed on ASOCT
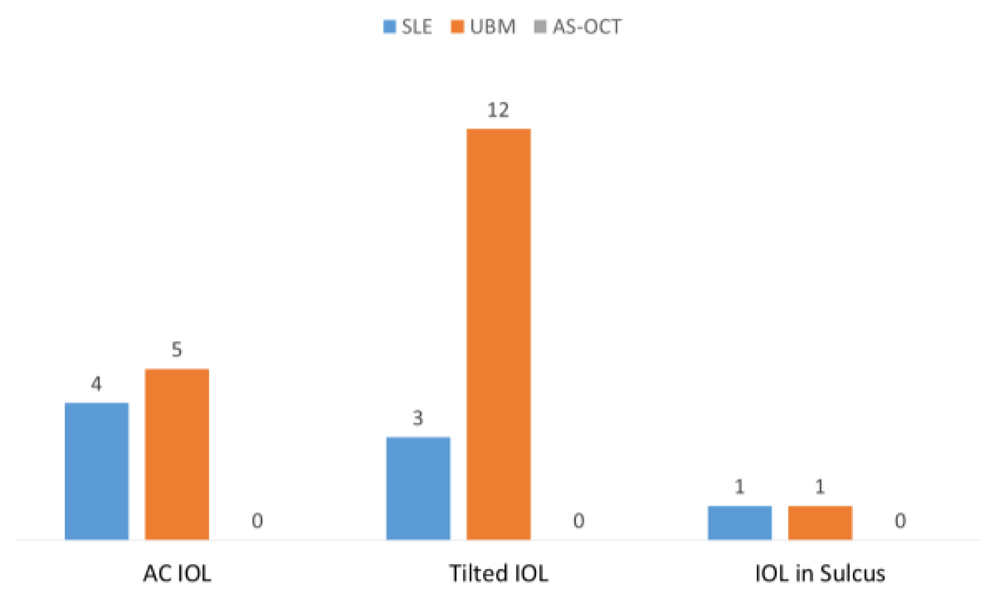
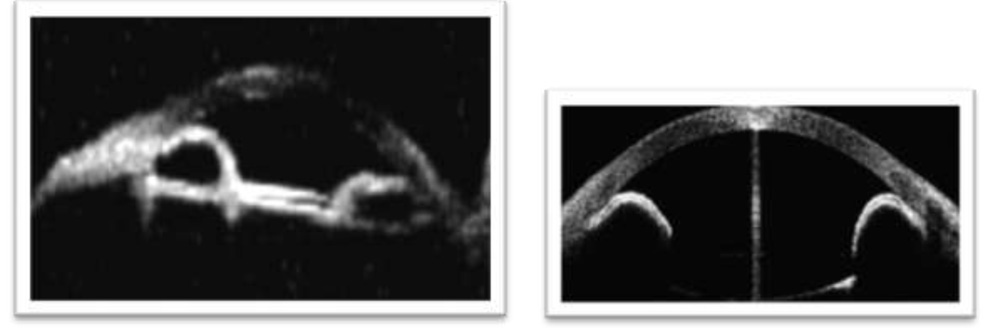
Figure 5 (a & b): Iris bombe on UBM and ASOCT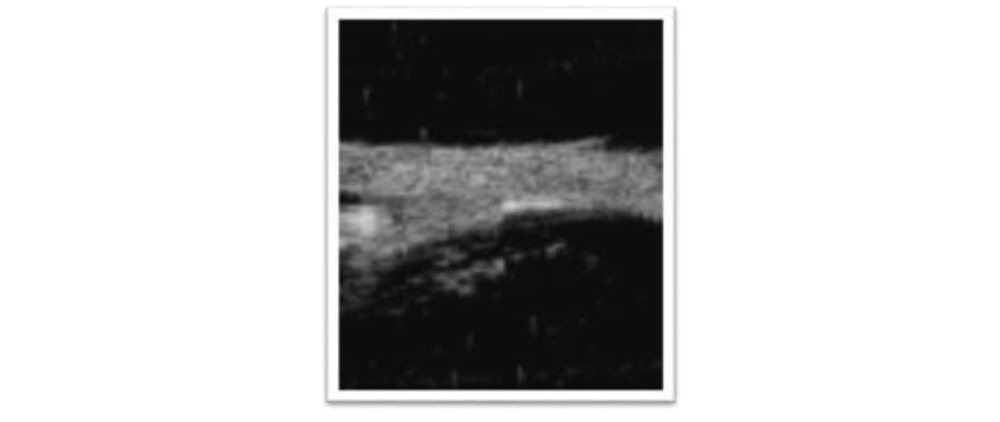
Figure 6: Exudates over pars plana on UBM