Dr. Benu Dubey, D06672, Dr. Dubey A K
Introduction
PDR is less aggressive in presence of posterior vitreous detachment.This fact has been mentioned in ETDRS and DRS. OCT and B scan were not available for clinical use at the time when the ETDRS and DRS trials were concluded. It was only through clinical observation that PVD was diagnosed. Documentation of PVD in a given case was not possible.These studies relied on clinical signs including disc pallor as end point of PRP. Angiographic documentation of regression of new vessels was not done either. Disc pallor means consecutive optic atrophy with corresponding field changes. These studies recommended 1600 to 3000 burns of 500 u size. Is it that we are doing excessive laser to meet the clinical end points?Is it possible to quantify the dose of laser with respect to pre existing PVD or that induced during treatment? These are the questions some of the questions we tried to answer in this study. Laser is known to induce PVD and present day drug treatment by way of intra vitreal injections also contributes to PVD.
Materials and Methods
Eighty eyes of forty patients with comparable status of PDR were registered for this study. The exclusion criterion were any previous laser treatment or intra vitreal drug treatment in the preceding six months. Only patients in whom ocular media permitted good fundus view were included. All eyes were subjected to detailed ocular examination,FFA(fundus fluorescein angiography) and OCT (optical coherence tomography) before starting treatment. Eyes with aggressive new vessels or visually significant macular edema were given intra vitreal Bevacizumab before starting laser.
Only 500 to 1200 laser burns of 200 u size were initially applied specifically covering the areas of capillary non perfusion. Weekly follow up was maintained for three months and at each visit OCT, B scan was done to monitor the vitreoretinal relation. In cases where PVD was present or occurred during the treatment careful follow up was maintained. All cases were subjected to FFA at eight weeks after laser to see the status of new vessels. Cases showing regression of PDR were not subjected to further laser, cases with active NV were subjected to further laser application.
Observations
Out of 80 eyes,16 eyes were detected to have either complete or partial PVD at first presentation. Among the remaining 64 eyes, 7 eyes started showing PVD in two weeks after anti VEGF and laser treatment, while 8 eyes showed partial or complete PVD over three weeks to four weeks with laser application alone. The group of eyes with existing or induced PVD included a total of 31 eyes(A), while the group without PVD included 49 eyes(B).
FFA done at eight weeks in either groups demonstrated regression of active NV in 24 eyes in group A ,with average laser burns from 800 to 1200 with 200 u size. In group B only 9 eyes responded in similar manner, remaining 40 eyes were further treated with laser variably. Figures 1,2,3,4 show OCT and FFA findings before and after treatment in a demonstrative case.
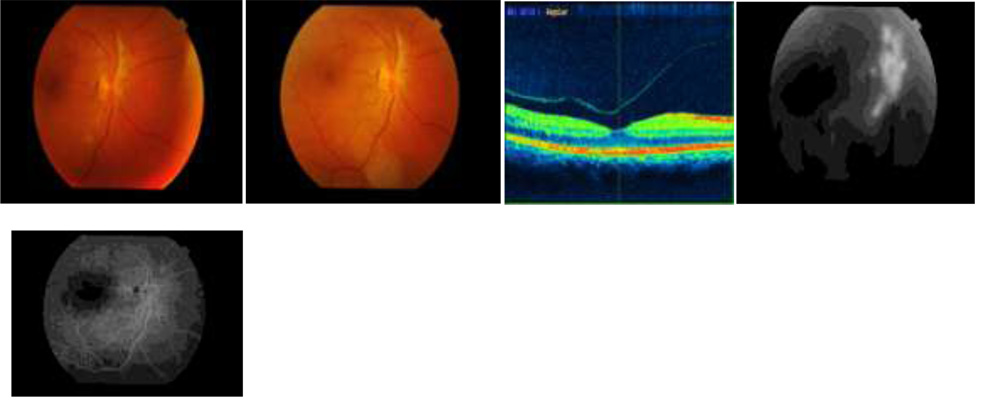 Fig. 1 Pre treatment color picture with pre retinal bleed, Fig.2 after rest Fig. 3 Pre treatment OCT showing PVD, Fig.4 Pre treatment FFA showing large NVD Fig.5 showing complete regression of NV at 8 weeks.
Fig. 1 Pre treatment color picture with pre retinal bleed, Fig.2 after rest Fig. 3 Pre treatment OCT showing PVD, Fig.4 Pre treatment FFA showing large NVD Fig.5 showing complete regression of NV at 8 weeks.
Discussion
Progression of new vessels is intimately related to vitreo retinal status in diabetic retinopathy. Trials are on for drug vitreolysis which will prevent possibly all complications of PDR including recurrent vitreous bleeding and TRD. At present a combination on anti VEGF drugs and laser PRP is the standard treatment for PDR.The limits of PRP as defined by ETDRS/DRS are disappearance of haemorrhages, exudates, narrowing of blood vessels and disc pallor.This means consecutive optic atrophy. OCT and B scan were not available at the time of ETDRS and DRS. With present tools to document and monitor vitreo retinal relation, it is shown in this study that nearly one third of laser dose is needed to regress new vessels.