Dr.RutiKa Khadse, K17013, Dr. Neelam Pawar, Dr.Padmavathy Maharajan, Dr. Meenakshi Ravindran
Presenting author: Dr Rutika Khadse
Co Authors: Dr. Meenakshi Ravindran
Dr. Padmavathy Maharajan
Dr. Neelam Pawar
 Introduction:
Introduction:
Optic neuritis (ON) can be defined as a pathologic process whereby inflammation of one or both optic nerves leads to visual dysfunction. Optic neuritis can be a presenting symptom of various inflammatory conditions and pediatric CNS demyelinating disorders and may be associated with dramatic visual loss. Idiopathic and postinfectious optic neuritis are more common in pediatric patients.(1) It is widely accepted that in children, attacks of optic neuritis usually occur following a febrile illness, tend to affect both eyes, are frequently associated with swollen discs, improve rapidly, and have a low conversion rate to multiple sclerosis (MS). Still there are varying differences in the studies done previously(2,3,4,5,6). In addition to that it is well known that genetic and environmental factors play an important role in the prevalence and clinical expression of demyelinating diseases (6).
Materials and Methods:
The records of all children <16 years of age diagnosed with ON from the period of January 2005 to December 2010 were retrospectively reviewed. The clinical diagnosis of ON was made on the basis of acute or subacute visual loss of 2 weeks or less, an afferent pupillary defect, and colour vision defect with or without optic nerve swelling, field defects, abnormal VEP. Information about age, sex, initial best-corrected visual acuity (VA), therapy, final best-corrected visual acuity, magnetic resonance imaging (MRI), and associated systemic disease was obtained. In all cases, the recovered VA was the final VA. Patients with hereditary optic neuropathy, systemic vasculitis, and malignancy were excluded from the study. Optic neuritis was classified as unilateral or bilateral. Patients were considered to have bilateral ON if involvement of both eyes occurred within 2 weeks of each other. Intravenous corticosteroids followed by tapering doses of oral steroids were given to all children.
Statistical analysis:
The data was collected and entered onto the Microsoft excel 2007 spread sheet. Mean (SD) and frequency (percentage) were used to describe the summary data. The statistical analysis was done by STATA 11.1 (Texas). P value less than 0.05 was considered as statistically significant.
Results:
We included 62 eyes of 40 children, with mean age of presentation of 11.5±3.2 years, ranging between 1 year to 15 years of age. There was female prepordance in our study with 27 (67.5%) females.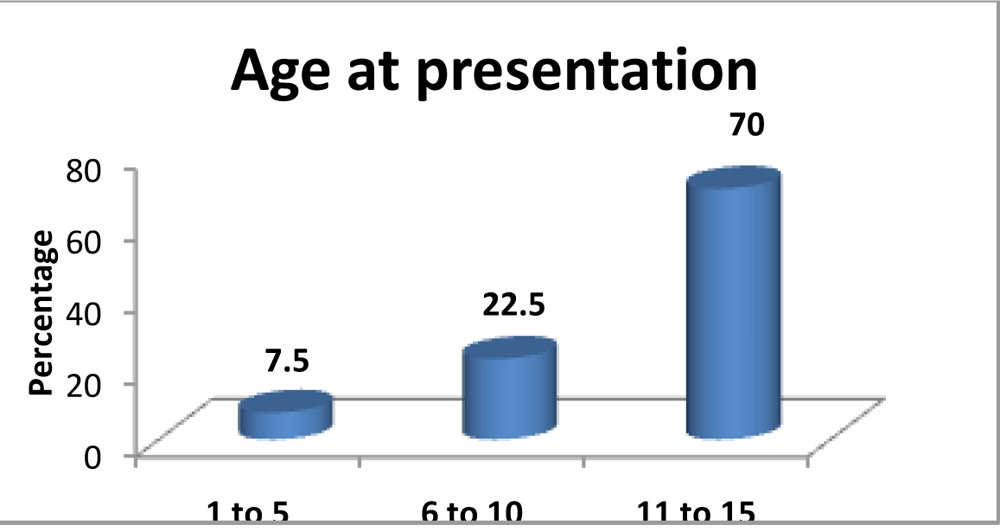 Table no. 1shows the visual acuity at presentation and final visits. Initial visual loss was severe (worse eye less than or equal to 6/60) [20/200)] in 35 eyes (57%). 10 of 62 eyes (16%) presented with visual acuity better than 6/12 [20/40]. 86% (53eyes) achieved final visual acuity better than 6/12 [20/40] , while 11% (7 eyes) still had visual acuity worse than 6/60 [20/200] at final visit.
Table no. 1shows the visual acuity at presentation and final visits. Initial visual loss was severe (worse eye less than or equal to 6/60) [20/200)] in 35 eyes (57%). 10 of 62 eyes (16%) presented with visual acuity better than 6/12 [20/40]. 86% (53eyes) achieved final visual acuity better than 6/12 [20/40] , while 11% (7 eyes) still had visual acuity worse than 6/60 [20/200] at final visit.
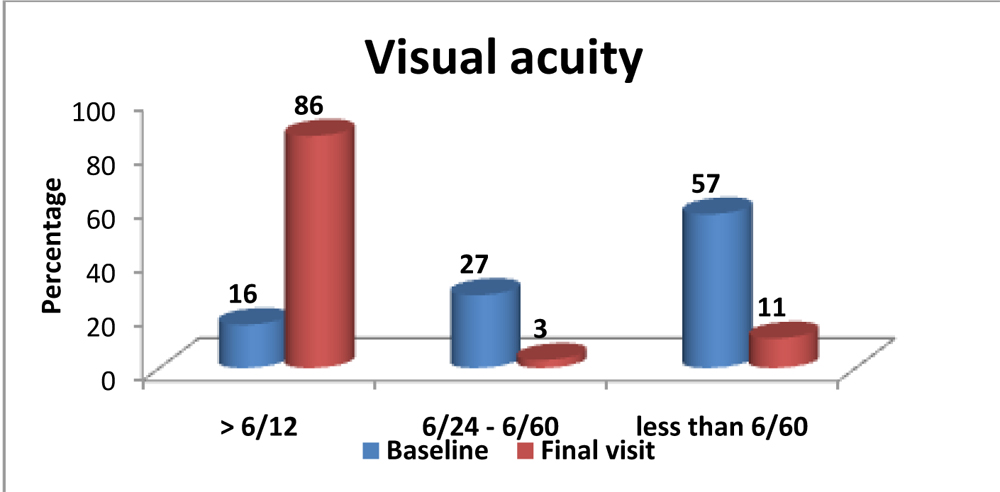
Graph no.2 showing comparison of visual acuity at presentation and at final visits.
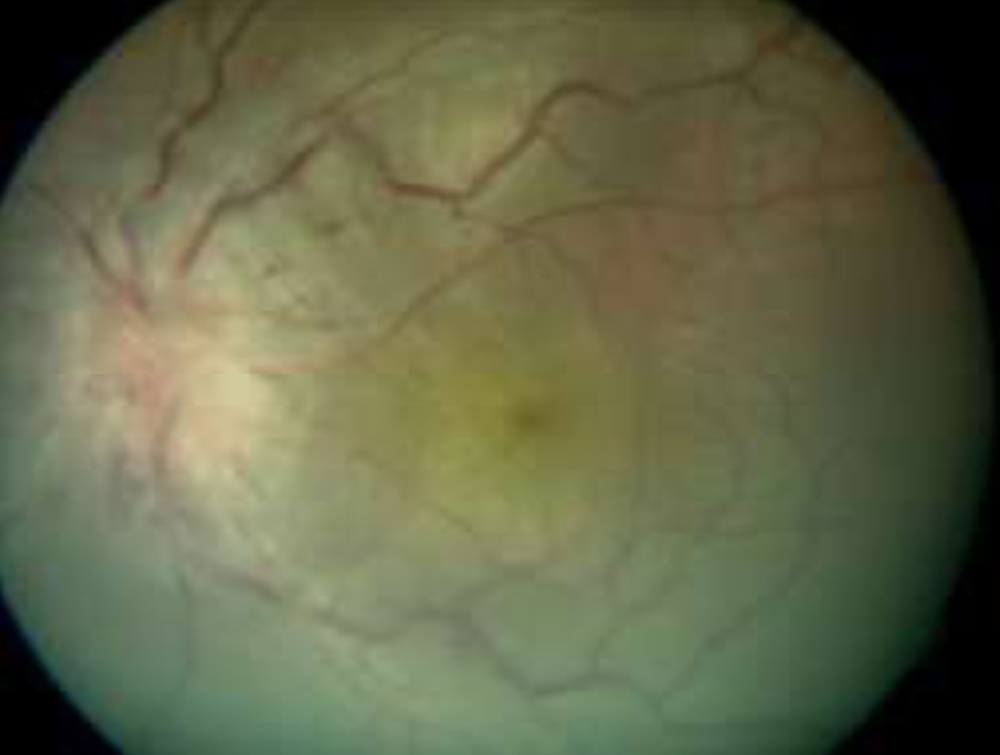
22 children (71%) had bilateral simultaneous involvement of optic nerve while it was unilateral in 18 (29%) children. Fundoscopy revealed papillitis in 61% (38 eyes), 39% (24 eyes) were associated with normal fundus. 3 of 40 children had recurrent episodes of optic neuritis. 7 (18%) of 40 children had preceding febrile illness within 2 weeks of presentation.
We had 1 patient with associated bilateral maxillary sinusitis, 1 had septicaemia and 1 was diagnosed to have acute disseminated encephalomyelitis(ADEM).
MRI brain was abnormal in 25 children of whom 14 children showed isolated optic nerve enhancement, 3 children showed demyelinating focus in frontal lobe and 3 children had similar hyper intensity focus including parieto-occipital lobe. None of them has developed multiple sclerosis till date. 4 (10%) of 40 children were diagnosed as multiple sclerosis developing demylination of various structures of brain including periventricular white matter, sub cortical structures, internal capsule, thalamus, structures of optic pathway including optic chiasma, optic tracts, optic radiation. 1 of the child had MRI suggestive of meningitis which later was diagnosed to have tuberculous meningitis.
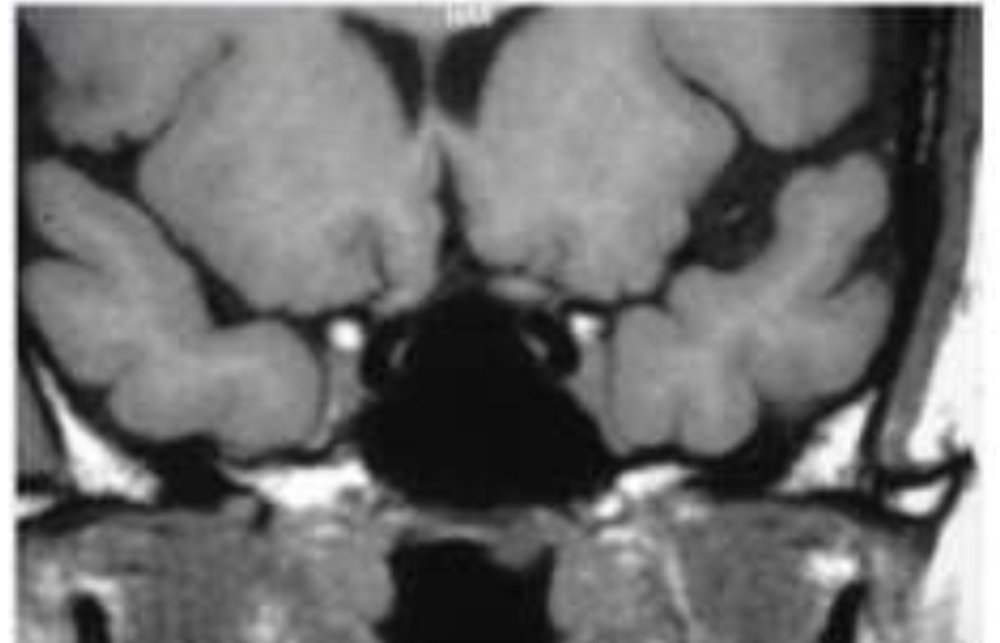 Image: 1a Optic chaisma: T1 weighted image
Image: 1a Optic chaisma: T1 weighted image
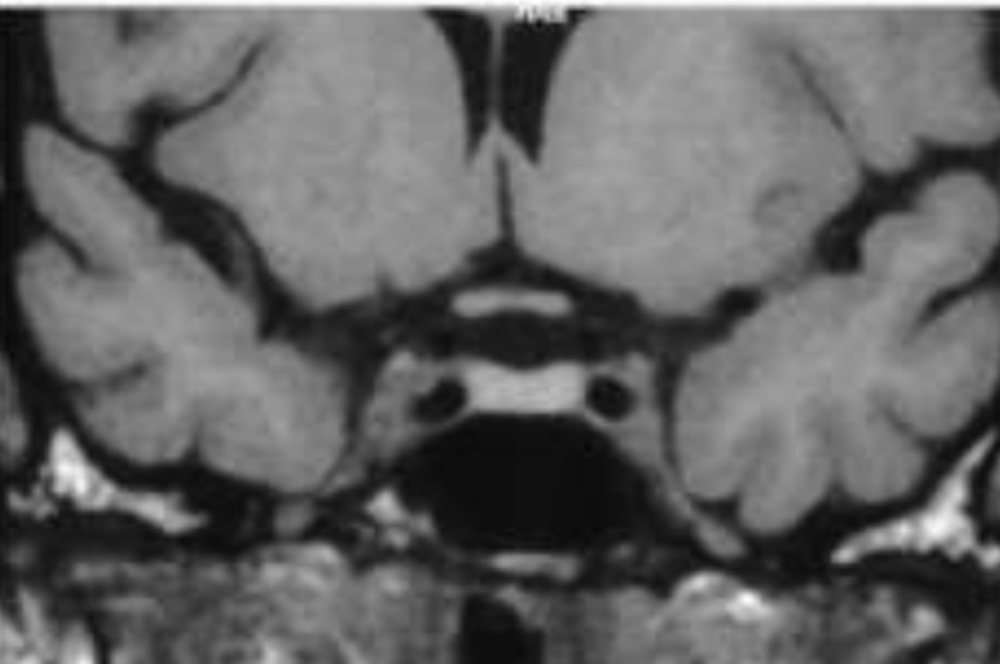 Image 1b T2 weighted image
Image 1b T2 weighted image
In 15 children (37%) MRI brain was normal. 1 of the child with normal MRI and recurrent optic neuritis was later diagnosed as having neuromyelitis optica with positive NMO aquaporin 4 (AQP4) antibodies. It was associated with very poor visual prognosis.
Visual evoked potential (VEP) was done in 7 children, in whom MRI brain was normal and presenting visual acuity was better than 6/12 (20/40) which showed latency of P100 waveform.
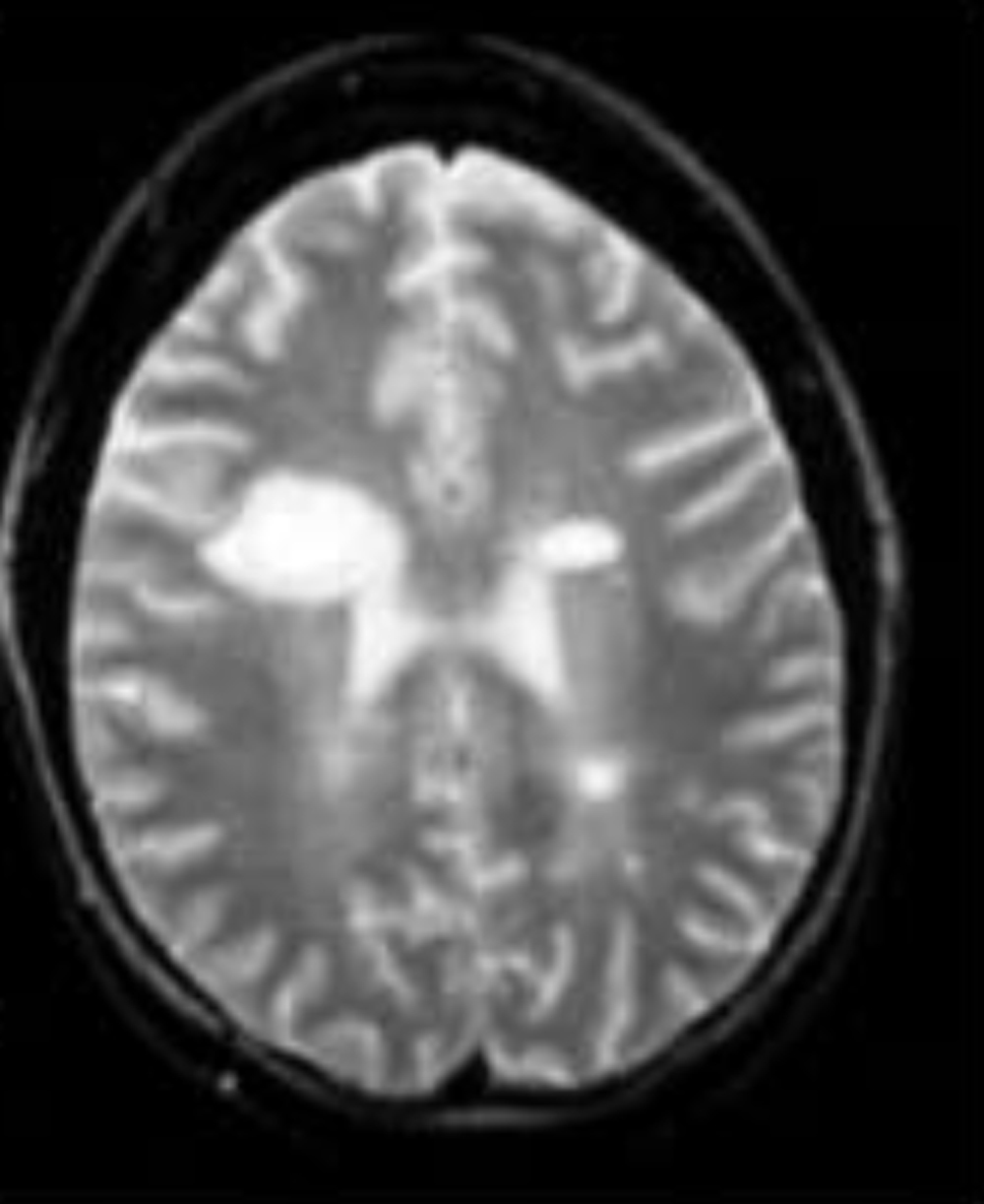 Image 2: Multiplehyperintensity lesions including brain parenchyma
Image 2: Multiplehyperintensity lesions including brain parenchyma
Discussion:
We studied the clinical characteristics, neuroimaging findings and visual outcome of paediatric optic neuritis in South Indian population.
Table No. 2 shows the comparison of various features of paediatric optic neuritis with previous reports.
Compared to data in previous studies many findings were similar but there were few differences in results of our study. The rate of involvement of girls was (67% in our study vs 43-60%)(2,3,4), disc swelling was present in (61% in present study vs 42-67%)(2,3,4), preceding febrile illness was present (18% in our study vs 28%-66%)(2,3,4) . Development of MS was lower in our study (10%) and other study done by Weiljto et al(3) (4%) as compared to previous case series (26%-36%)(2,4)
Wilejto(3) and colleagues found that bilateral optic neuritis was associated with an increased risk of MS, regardless of the age at presentation, while we had 4 cases of MS of which 3 had unilateral vs 1had bilateral presentation for MS. A systematic review and meta-analysis of optic neuritis in children done by Waldman et al(5), showed that the presentation (bilateral vs unilateral) is not a factor in the development of MS.
The risk of MS in children presenting with optic neuritis and abnormal brain MRI scans, after adjustment for age, was significantly greater than for children with unremarkable brain MRI scans in study done by Waldman(5), while in present study of 25 abnormal brain scans only 4 (16%) children developed MS.
The differences in the findings could be due to varied period of follow up and racial differences as the study were done in different populations.
Conclusion:
Paediatric optic neuritis is more likely to be bilateral and associated with good visual recovery. Neuroimaging plays important in role in diagnosing other conditions associated with optic neuritis.
| VA category | Baseline | Final visit |
| > 6/12 | 10 (16%) | 53 (86%) |
| 6/24 – 6/60 | 17 (27%) | 2 (3%) |
| less than 6/60 | 35 (57%) | 7 (11%) |
| Total | 62(100) | 62(100) |
Table no.1: showing visual acuity at presentation and after final recovery.
| Present study 2016 | Wieljito et al(3) | Hwuang et al(2) | Morales et al(4) | |
| No. Of patients | 40 | 36 | 23 | 15 |
| Age distribution | 1-15 | 2.2-17.8 | 3-15 | <15 years |
| Mean age of presentation | 11.15 | 12.2 | 8.9 | 9.8 |
| Females | 67% | 58% | 43% | 60% |
| Bilateral | 71% | 42% | 87% | 66% |
| Preceding febrile illness | 18% | 28% | 39% | 66% |
| Final v/a >6/12 | 86% | 83% | 79% | 58.3% |
| Final v/a worse than 6/60 | 11% | 4% | 30% | |
| Disc swelling | 61% | 67% | 42% | 64% |
| MS | 10% | 36% | 4% | 26% |
| Focal demyelinating lesions | 25% | 54% | 4% | 33% |
Table no.2 : comparing the various characteristics with the previous reports.
References:
- Jennifer Graves, Verena Kraus, Bruno P. Soares, Christopher P. Hess and Emmanuelle Waubant. Longitudinally Extensive Optic Neuritis in Pediatric Patients; Journal of Child Neurology.2015, Vol. 30(1) 120-123
- Jeong-Min Hwang, Yong Jae Lee, and Mee Kum Kim Optic Neuritis in Asian Children.Journal of Pediatric Ophthalmology and Strabismus 2002; 39:26-32.
- Wilejto; M. Shroff, J.R. Buncic, J. Kennedy, C. Goia, B. Banwell. The clinical features, MRI findings, and outcome of optic neuritis in children. NEUROLOGY 2006;67:258–262
- Morales DS, Siatkowski RM , Howard CW , Warman R.Optic neuritis in children. Journal of Pediatric Ophthalmology and Strabismus [2000, 37(5):254-259]
- Waldman, Lindsey B. Stull, Steven L. Galetta, Laura J. Balcer, and Grant T. Liu et al. Pediatric optic neuritis and risk of multiple sclerosis:Meta-analysis of observational studies ; J AAPOS 2011;15:441-446
- Marco Aurélio Lana-Peixoto, Gustavo Cardoso de Andrade. The clinical profile of childhood optic neuritis. Arq Neuropsiquiatr 2001;59(2-B):311-317