Dr. Mona Gautam, G17154,
Dr.Manjunath Natarajan,
Dr. H Niveditha
AIOS Free Paper FP980
CHIEF AUTHOR / PRESENTING AUTHOR
DR MONA GAUTAM
CO AUTHORS:
- DR. H NIVEDITHA
- DR. MANJUNATH NATARAJAN
ABSTRACT
Background
Cataract surgery is the most common surgical procedure performed in ophthalmic units. Many patients who have undergone cataract surgery have complained of dry eye and symptoms of irritation post operatively. The dry eye following cataract surgery may be induced surgically or by excessive instillation and incorrect use of eye drops with preservative. Patients with DM are at higher risk to develop cataract than Non DM patients. The present study aimed at analyzing the effects of SICS on various parameters of dry eye.
Objectives
- To assess the effect of SICS on tear film stability, tear secretion and dry eye symptoms in diabetics and control group.
- To provide appropriate treatment as and when required
- To find out the factors which may be influencing the symptoms and test results.
Study Design
One and a half year, Comparative hospital based study
Methods
A comparative hospital based study conducted on 150 eyes of 150 patients admitted in KIMS Hospital and Research Centre, Bangalore for SICS. Written consent, after explaining the procedure, were taken after fitting inclusion and exclusion criteria. Data collected included demographic details, pre op evaluation (ocular and systemic examination and investigation which are pre requisite for cataract surgery) and detailed tear film evaluation including biomicroscopic examination of tear film like TBUT and TMH, Sch 1 and biomicroscopic examination of conjunctival staining using LG and FS respectively.
Results
In the present study 150 eye of 150 patients above 40 years of age undergoing SICS were selected. Both DM and Non DM group showed increased dry eye symptoms during 1st Post operative week. Among Non DM patients, dry eye symptoms increased from 9.3% to 29.3% in 1st week post operatively which decreased subsequently. In DM, 30.7% of patients showed dry eye symptoms pre operatively, which increased to 64% during 1st week post operatively and during 6th week, it came down to 36%. TBUT among Non DM decreased from 16.91 Sec to 8.60 sec in 1st week.
It increased during 6th week post OP to 10.41 sec. Among DM, TBUT showed decrease from 13.12 sec to 5.04 during 1st week post OP which improved subsequently. In both DM and Non DM, P (<0.001) value showed strong correlation. Sch 1 Test values among Non DM showed no significant result as observed pre and post SICS values fall within normal range. Among DM value of Sch1 showed moderate correlation with pre OP values. During 1st week Sch1 value decreased to 7.23 mm from its pre OP value of 17.77 mm. FS and LG showed marginal deterioration post operatively with no significant result. TMH among Non DM and DM groups showed no correlation between pre operative and post operative values.
Conclusion
Dry eye symptoms and signs developed after SICS with peak severity on
day 7 and improved over time. The dry eye pattern was similar between all three clinical tests (TBUT, Sch 1 and Oxford ocular staining system) and dry eye symptoms. Diabetic patients suffer more damage to tear film which is not only from diabetes but also from surgery. However it is important that ophthalmologist assess dry eye before and after SICS to ensure proper treatment, quality of vision and quality of life for patients.
Key words
Dry eye; Diabetic; SICS; Sch 1; TBUT; TMH; FS; LG.
INTRODUCTION
Dryeye is a multifactorial disease of the tears and ocular surface that results in symptoms of discomfort, visual disturbance and tear film instability with potential damage to the ocular surface. It is accompanied by increased osmolarity of the tear film and inflammation of the ocular surface. Damage to any component of lacrimal function unit can destabilize the tear film and lead to ocular surface disease.1
Lacrimal function unit comprises of lacrimal gland, ocular surface (cornea, conjunctiva and meibomian gland), lid, sensory and motor nerve that connect them.2,3
Using the Indian definition of blindness, cataract is responsible for 77.5% of all blindness and 84.4% of avoidable blindness.4 At the same time, cataract surgery is the most classic and successful surgery in field of ophthalmology. According to National Programme for Control of Blindness 2010-11, cataract operations have increased to 59.1 lakh during 2009-10 from 16 lakh during 1992. In our hospital most common surgery done is SICS which is effective and economical.
Numerous epidemiological studies have reported that ageing, connective tissue disease, history of allergy or diabetes and use of antihistamines and ocular surgery are risk factors for development of dry eye syndrome.
Diabetic patients experience higher rate of corneal and ocular surface abnormalities like corneal erosion syndrome, persistent epithelial defect, delayed wound healing and corneal scar/opacity . Location and shape of surgical incision and additional factors like topical anaesthesia, preservative eye drops used in cataract surgery may add to an already compromised and neurotrophic cornea. These can affect surgeon’s approach to surgery as well as post operative management.5 The possible mechanism contributing to tear dysfunction are diabetic neuropathy results in neutrophic cornea and/or vascular changes in lacrimal gland.
Ocular surface disorder is one of the post operative complication developed following SICS which disturbs visual outcome. Mechanism is as follows:2
- Chronic use of eye drop after cataract- preservative can lead to corneal and conjunctival toxic changes.
- Tear film instability at the site of incision causes faster tear breakup time and decreased mucin production.
- Exposure to bright light of microscope during surgery
- Decreased corneal sensation
To maintain ocular surface is important for better visual outcome after cataract surgery. This can be achieved by early diagnosis and treatment.
It is significantly important for maintaining of the ocular surface stability and recovery of visual acuity after cataract surgery to do early diagnosis and promptly manage the dry eye syndrome.
AIMS AND OBJECTIVES
1. To assess the effect of SICS on tear film stability and tear secretion in diabetics and control group.
2.To assess the dry eye symptom and tear film abnormalities in diabetics and control group during post operative period (till 6th week)
3.To find out the factors which may be influencing the symptoms
4.To assess tear film diagnostic tests results in pre and post operative periods.
5.To give appropriate treatment as and when required.
REVIEW OF LITERATURE
Onsiri Thanathanee et.al. in article “How diabetes impacts the Cornea and Ocular Surface” reported that Ocular surface disease is one of several important problems to consider in diabetic patients with cataract, especially dry eye with a dysfunctional tear state. Corneal sensitivity and tear function tests were both decreased. Both preoperative and postoperative dry eye disease are well established in studies of diabetic patients and can initiate postoperative ocular surface problems such as recurrent corneal erosion syndrome, persistent epithelial defect, delayed wound healing and corneal scar/opacity. Careful preoperative ocular surface examination and aggressive treatment before surgery may alleviate signs and symptoms, including complications of postoperative dry eye disease in diabetic patients undergoing cataract surgery.5
Vasilis Achtsidis et. al. in the article “Dry Eye Syndrome in Subjects With Diabetes and Association With Neuropathy Diabetes Care” reported that diabetes mellitus has been identified as a risk factor for dry eye syndrome (DES). The prevalence of DES in diabetes has been reported to be upto54.3%. The cornea is one of the most densely innervated parts of the human body containing myelinated A-d and unmyelinated C fibers, deriving its innervation from the ophthalmic division of the trigeminal nerve. The study suggested that patients with polyneuropathy have corneal nerve fiber damage and reduced corneal sensitivity. The study concluded that DES is particularly common in patients with type 2 diabetes who have polyneuropathy, and it is associated with reduced corneal sensitivity. Corneal hypoesthesia reduces patient’s symptoms, and DES might be asymptomatic and insidious. They suggested that patients with polyneuropathy be screened for DES and probably treated long-term for the prevention of ocular surface damage.6
Xi Liu et.al conducted a study on 47 patients to evaluate tear film stability and tear secretion in patients with diabetes after phacoemulsification. The study showed that diabetics had a decreased preoperative TBUT and Sch 1. TBUT was reduced on Day 1 and recovered on Day 180 postoperatively in both groups. Sch 1 was increased after phacoemulsification, but returned to preoperative levels by Day 180 in non-diabetics, whereas it was lower than preoperative level in diabetics. Positive corneal fluorescein staining was elevated in both groups, and returned to preoperative levels only in controls. Dry eye symptoms were similar to fluorescein staining in both groups. This study concluded that tear secretion was reduced in diabetic cataract patients after phacoemulsification, which worsened dry eye symptoms and predisposed those patients to ocular damage.7
Nora Burda et.al conducted a study on 223 patients to analyze the correlation of Dry Eye and Diabetes Mellitus Type II. The study showed that dry eye is a disorder of tear film because of tear deficiency or excessive tear evaporation which causes damage to the inter palpaberal ocular surface and is associated with symptoms of ocular discomfort. Above study concluded that prevalence of Dry Eye was significantly higher at patients with longer duration of diabetes. The study concluded that dry eye seems to be an important contributing factor related to corneal abnormalities. Age and sex does not seem to play any important role in this condition. Good glycemic control is important for prevention and control of dry eye syndrome.8
Sun XG et al. has reported that most cases of early dry eye, who usually had the normal lacrimal secretion before surgery, were reversible and involved in some of factors associated with surgery and post-surgery medication. But most cases of chronic dry eye, who have abnormal lacrimal secretion or “borderline state” of lacrimal secretion test before surgery, may suffer from the ocular surface diseases related to irreversible dry eye disease. It is significantly important for maintaining of the ocular surface stability and recovery of vision acuity after cataract surgery to do early diagnose and promptly manage it.9
Li XM et.al. conducted a study on 37 patients to investigate dry eye in patients before and after cataract surgery. Study showed that after cataract surgery, the incidence of dry eye increased dramatically. Tear river was narrowed, TBUT and Sch 1 were decreased and shorted in patients after cataract surgery. Dry eye can be induced or deteriorated after cataract surgery, if it cannot be treated on time.10
Oh T. et al. conducted a study on 30 patients to evaluate changes in the tear film and ocular surface after cataract surgery. The study concluded that microscopic ocular surface damage during cataract surgery seems to be one of the pathogenic factors that cause ocular discomfort and dry eye syndrome after cataract surgery.11
Yoon KC et al. conducted a study on 127 patients to investigate changes of tear film and ocular surface in diabetes mellitus. The study showed that the degree of keratoepitheliopathy was severe, and the corneal sensitivity, TBUT, and tear secretion were significantly reduced in the diabetic patients. All parameters were related to the status of metabolic control, diabetic neuropathy, and stage of diabetic retinopathy.12
THE TEAR FILM
Of all the components that constitute the lacrimal functional unit, the tear film is by far the most dynamic. It provides nutrients, a communication pathway, distributes regulatory factors and provides a pathway for cells to reach the epithelium. The tear film consists of a variety of different components, including electrolytes, salts, protein and peptides. Studies provide evidence that specific proteins or peptides in the tear film can be used as diagnostic biomarkers for dry eye, ocular surface diseases,13 and even certain systemic disease states, such as diabetes mellitus.14
The tear film has a number of specific functions:
1.It lubricates and nurtures the anterior tissues of the eye.
2.It provides a regular optical surface for the eye’s optical system, by filling the irregularities of the corneal epithelium.
3.Oxygen dissolved in the tear film is the only source for normal aerobic metabolism of the corneal epithelium and stroma.
4.It is an integral part of the ocular surface defense mechanism. It also functions as a method to remove cellular debris and metabolic waste from the cornea and conjunctiva.
The integrity and normal functioning of the tear film is maintained by a complex physiological mechanism, which includes adequate production of the various components by different glands, stability of the various layers on the ocular surface and timely drainage through the lacrimal ducts. Any disruption in the physiology or stability of the tear film may result in dry eye.
In 1946, Wolff 15 presented a classic description of the tear film, in which it was composed of a three-layered structure, consisting of an anterior lipid layer, middle aqueous layer and deeper mucin layer (Figure 1).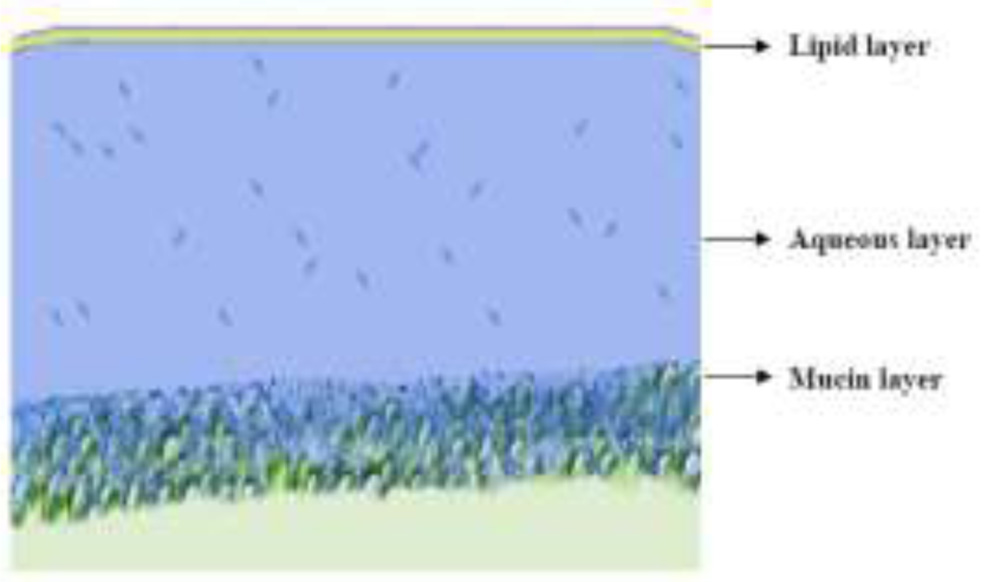
Another model with six layers has also been proposed by Tiffany,16 which included the original three layers proposed by Wolff, along with air-lipid, lipid-aqueous and aqueous-mucus interfaces. More recently it has been suggested that there are dissolved mucins in the aqueous layer, which decrease in concentration towards the lipid layer. The most currently accepted current concept is that the tear film is a bi layered structure, consisting of an aqueous/mucinous phase, with an overlying superficial lipid phase (Figure 2). However, despite the intervening 60 year period, the original 3 layered Wolff model is still accepted as being a valuable concept.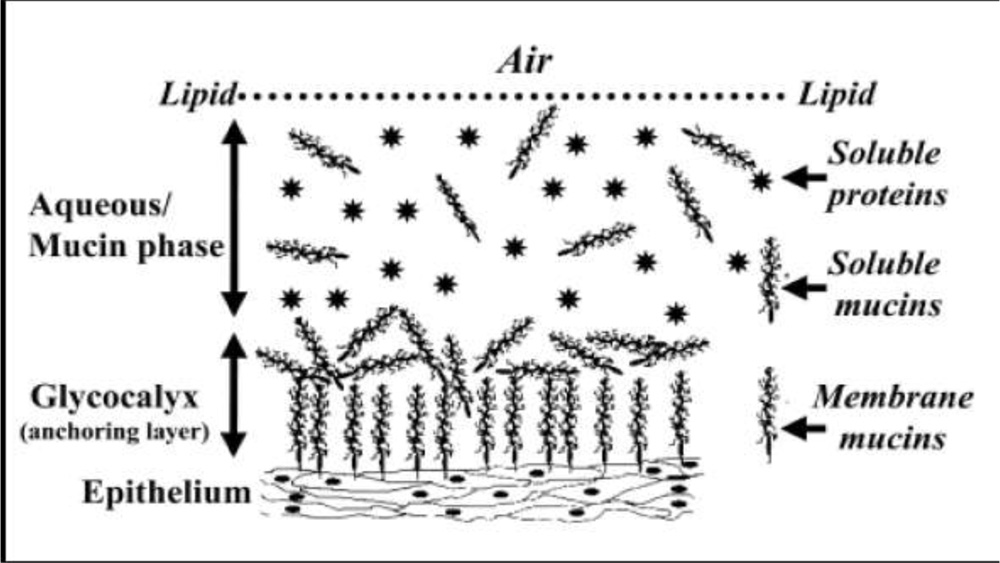
Figure 2: Proposed structure of precorneal tear film
The thickness of the tear film is vitally important to understand, because the thickness determines the tear volume from which evaporation occurs when the eyes are open. However, there is no agreement among researchers on the “true” thickness of the tear film. Various studies to investigate tear film thickness have been performed, using a variety of techniques, and these studies have quoted tear film thickness ranges from 1.5μm to 45μm.17-18 Prydal et al found the tear film thickness to be 34-45μm with coherence interferometry and confocal microscopy.17 More recently, King-Smith et al.,18 using wavelength dependent interferometry, have reported the thickness of the tear film to be 1.5-4.7μm in normal subjects.
LAYERS OF THE TEAR FILM 19
The lipid layer of the tear film
Lipid forms the superficial/outermost/ surface layer of the tear film and is derived primarily from the meibomian glands but also from the glands of Zeiss and Moll in the eyelids. The layer is an oily film, 0.1 μm thick. It consists of an outer non-polar lipid layer and an inner polar layer. The meibomian glands are richly innervated by both sympathetic and parasympathetic neurons. Androgen has an important role to play in the functioning of meibomian glands. It increases the size, activity and lipid production in the meibomian glands.20-21 Tear lipocalin enhances the stability and spreading of the lipid layer, which decreases the surface tension of aqueous by forming complexes with polar lipids.
Functions of the lipid layer
- To provide an effective barrier and prevent evaporation.
- To provide a surfactant layer that acts as an effective bridge between the non polar lipid layer and the aqueous mucinous layer.
- To act as a lubricant to facilitate the movement of the eyelids during blinking.
- To maintain compression and expansion of the lipid film during blinks, to prevent tear overflow.
- To form a barrier for preventing contamination of the tear film.
- To provide a smooth surface for refraction of the incoming rays of light. Defects and instability in the lipid layer can be responsible for tear breakup, with subsequent dry spots leading to dry eye.
Lipid dynamics and drainage22
With every down-phase of the blink, lipid is squeezed out of the meibomian glands and is compressed into the lid margins. On the up-phase of the blink, the lipid rapidly spreads upwards over the aqueous layer, suggesting that the lower eyelid reservoir is the major contributor to the spreading lipid. Most of the excretion of the lipid layer occurs by bulk flow over the lid margin and onward to the neighboring skin and lashes. Some of the lipid, mainly polar, mixes with the aqueous layer and is drained via the naso-lacrimal drainage pathway.
Composition of the lipid layer
It is believed that the lipid layer has two distinct regions. There is a relatively thick outer layer, containing non polar lipids such as wax esters, sterol esters, hydrocarbons, and triglycerides; and a thin polar inner layer, predominantly consisting of phospholipids. The polar phase of the lipid layer owes its surfactant properties which facilitate mixing with both aqueous and non-polar lipids It acts base for the more superficially located non-polar lipids. The major classes of lipids are the wax monoesters and sterol esters, which comprise approximately three-quarters of the meibomian gland fluid.
Physical properties of lipid
Although isolated meibomian lipids do not spread over saline, the lipid layer spreads well over the aqueous phase of the tear film. The refractive index of the lipid layer varies with wavelength and temperature.
Tear lipids in dry eye
Analysis of lipid components has shown a considerable decrease in triglycerides and cholesterol, and monounsaturated fatty acids (specifically oleic acid), in patients with obstructive meibomian gland dysfunction, chronic blepharitis and viscous meibum. These changes in the lipid composition may be associated with tear film instability. Polar lipids may define the structural organization of the overlying non-polar lipids and loss of these constituents are believed to result in decreased tear breakup time and increased aqueous tear evaporation.23
The aqueous layer
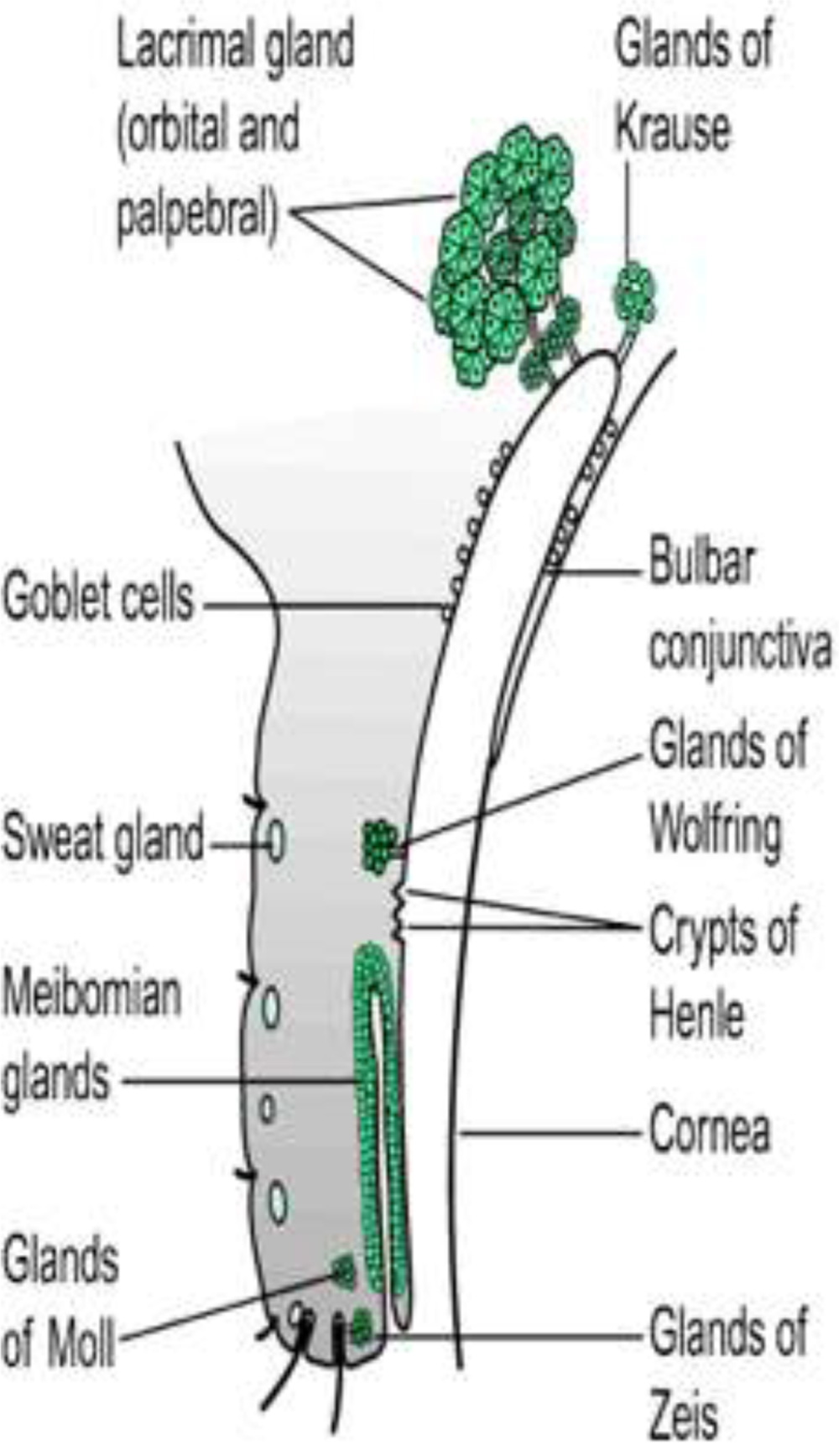
The aqueous layer of the tear film comprises the bulk of the tear film thickness. This intermediary watery phase of the tear film is approximately 6.5-7.5 μm thick and is mainly produced by the main lacrimal gland, and also by the accessory glands of Krause and Wolfring (Figure 3). It contains electrolytes, protein enzymes and metabolites.
AQUEOUS PRODUCTION
1.The lacrimal gland
The lacrimal gland, the main secretor of the aqueous phase of the tear film, is located in the upper outer part of the orbit in a shallow depression in the frontal bone and is divided into larger orbital and smaller palpebral lobes. The gland is a multi-lobed, tubulo-acinar structure with ducts that terminate at the surface of the eye in the lateral portion of the superior fornix.24
2. Accessory lacrimal glands
The accessory glands comprise the glands of Krause and Wolfring. There are more than 20 accessory glands of Krause in the upper conjunctival fornix and about 6-8 in the lower conjunctival fornix. Glands of Wolfring are found in the upper border of the tarsal plate.24
Components of the aqueous layer
The bulk of the aqueous component of the tears is not only composed of water, but contains numerous electrolytes, proteins, peptide growth factors, vitamins, antimicrobials, cytokines, immunoglobulins, and hormones. The composition of the tear film varies in response to environmental and bodily conditions. Electrolytes present in the tear film include sodium, potassium, magnesium, calcium, chloride, bicarbonate, and phosphate ions. These are largely responsible for modifying the osmolality of tears, act as a buffer to maintain pH at a constant level and maintain epithelial integrity.
Major tear proteins include lysozyme, lactoferrin, secretory immunoglobulin A (sIgA), serum albumin, lipocalin (previously called tear-specific pre albumin), and lipophilin. These proteins are secreted in response to an intracellular stimulus and the rate of secretion approximately matches the tear flow rate. Numerous peptide growth factors including EGF, HGF, TGF β are also found in the aqueous.
Functions of the aqueous layer:
1.This is quantitatively the most important layer.
2.It is responsible for creating a conducive environment for the epithelial cells of the ocular surface, carrying essential nutrients and oxygen to the cornea, allowing cell movement over the ocular surface.24
3.Lysozyme, lipocalin, lactoferrin and IgA are responsible for antimicrobial activity.
4.Washing away debris, toxic substance and foreign bodies.
5.Many of the growth factors that are present in the aqueous phase play a significant role in corneal physiology. 24
Physical properties of the aqueous layer
The normal pH value of the tear film is between 7.14 and 7.82, which is similar to plasma pH.25
Tear dynamics and drainage22
The tears are directed from the upper temporal fornix to the lacrimal puncta in different ways. Tears move downward by gravity at the lateral canthus to form the lower marginal tear strip, capillary attraction then moves tears into the punctum and vertical section of the canaliculus, and finally the lid movement during the blink forces the tears in the puncta. The rapid closure of the temporal end of the palpebral aperture during the blink aids the nasal movement of tears. The same blinking movement forces the tears into the lacrimal sac through the canaliculi from each of the lacrimal puncta. The lacrimal saccollapses after the blink due to the relaxation of the orbicularis, thus forcing the tears into the nasolacrimal duct. From the nasolacrimal duct, the tears are finally excreted into the nasal cavity. The basal tear production of the tear film is 1-2 μl/min and the turnover rate is approximately 16%/min in normal subjects.
Aqueous layer in dry eye
Lysozyme levels decrease with age and in dry eye syndromes.26 Sjogren’s syndrome patients show a decrease in lysozyme, lactoferrin and EGF levels in tears.27 Deficiency of tear lipocalin can lead to the formation of mucous strands and cause tear film instability. In a study of intolerant contact lens wearers, it was found that tear lipocalin concentration was significantly elevated compared to a control group of tolerant wearers. The concentration of Aquaporin 5 (AQP5), which is a selective water channel protein, was significantly increased in tears of Sjogren’s syndrome patients, compared with normal controls.28
3 The mucous layer
Production of the mucin layer
The primary source of tear film mucins is from the goblet cells of the conjunctiva and the crypts of Henle in the conjunctival fornices. A secondary source of mucin is from the squamous epithelial cells of the ocular surface (cornea and conjunctiva), with a small contribution from the lacrimal gland. Goblet cell mucin forms a gel in the deepest layer of the tear film, while soluble mucin is found in the aqueous layer. Ocular mucins influence the tear-film break up time and play a major role in stabilizing and spreading the tear film, and also play a major lubrication function.29
Functions of the mucin layer
There are several key functions of the mucin layer, which include:
1.The most important function of mucin is lubrication, facilitating the eyelid margins and palpebral conjunctiva to slide smoothly over one another during blinking and ocular rotational movements.
2.The corneal surface is wettable, however when non-wetting occurs in areas of the cornea, mucus plays an important role in overcoming this hydrophobicity.
3.Mucus threads cover foreign bodies with a slippery coating, protecting the cornea and conjunctiva from abrasion.
4.Mucus also helps in wetting the ocular surface and in glycocalyx formation.
5. The ocular surface glycocalyx acts as a barrier to pathogens.
Composition and properties of mucins 29
Mucins are defined as high molecular weight glycoproteins, that have at least 50% of their mass is carbohydrate, O-linked to serine and threonine residues present within tandem repeats of amino acids in their protein backbone. They are hydrophilic in nature. The carbohydrate chains account for about 70% to 80% of the dry weight of mucins. The molecular mass of mucins range from 3 × 105 to over 4 ×107 kDa.
To date, at least 20 distinct human mucins have been cloned (MUC1– MUC20,including 3A, 3B, 5AC, and 5B). Mucins are classified as either trans membrane or secretory mucins.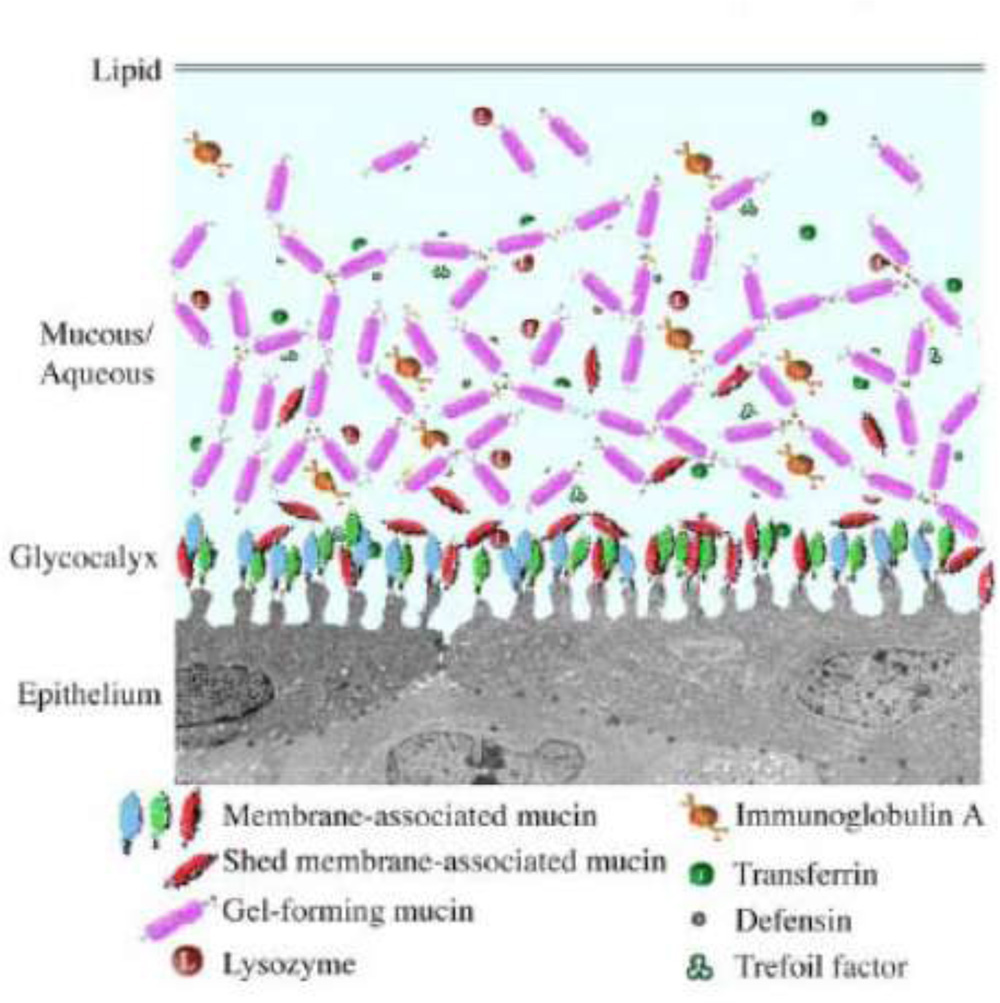
1.Transmembrane mucins
Transmembrane mucins contain hydrophobic, membrane-spanning domains in their carboxyl-terminal region, which anchor them to the apical surface of conjunctival and corneal epithelial cells, facilitating formation of the ocular surface glycocalyx. MUCs 1, 3A, 3B, 4, 12, 13,15, 16, 17 and 20 have been characterized as membrane associated. 31
2.Secretory mucins
The gel-forming mucins are the largest glycoproteins known, with genes of 15.7 to 17 kb and deduced proteins of approximately 600 kDa. The hydrophilic character of secreted mucins, which results from their heavy glycosylation, helps to hold fluids on epithelial surfaces. Secreted mucins can be further sub-classified as gel-forming or soluble, based on their ability to form polymers.MUC 2, 5AC, 5B, 6,7 and MUC9 are classified as secretory mucins.
Mucins in dry eye syndrome
Studies indicate that mucin gene expression and translation, as well as mucin post translational processing are affected in dry eye conditions.30 Real-time quantitative PCR has shown a significant decrease in RNA transcripts for MUC5AC in the conjunctival epithelium of patients with Sjogrens syndrome, compared with normal individuals. Protein levels of MUC5AC assessed by ELISA are also significantly reduced in the tear fluid in dry eye. Alterations in membrane-associated mucins are noticed in non-Sjogren’s syndrome dry eye and Sjogren’s syndrome dry eye.
Control of Tear Secretion32
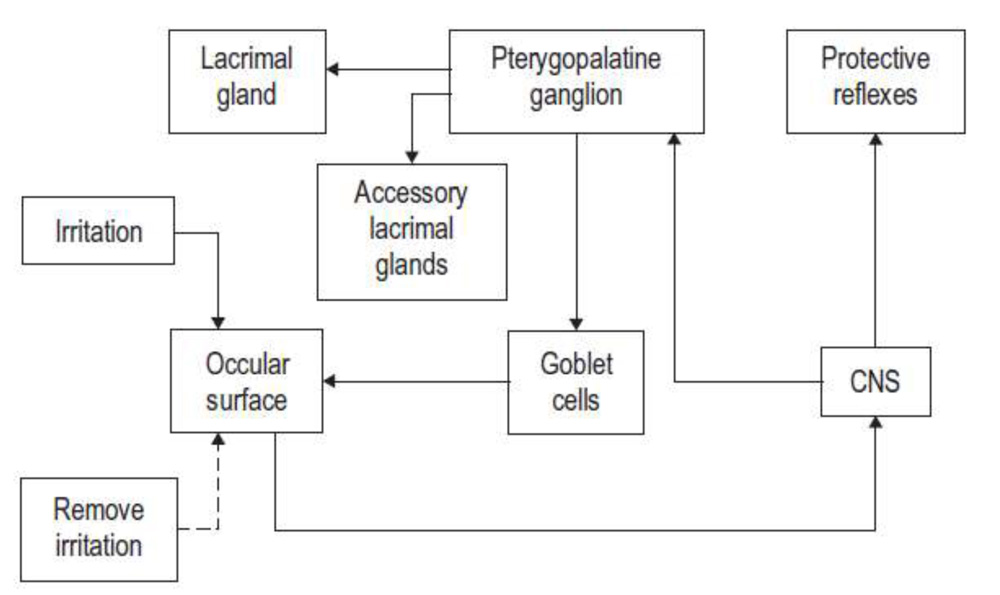
Figure 5: Flow chart representing control of tear secretion
The small sensory nerve endings located just below the epithelial surface of the cornea, lid margin, and conjunctiva constantly respond to drying and temperature change as well as contact and chemical changes, by sending intensity-coded neural signals to the spinal trigeminal nucleus located in the brain stem. A multisynaptic pathway to the preganglionic parasympathetic nuclei in the superior salivatory nucleus forms the output to the secretory tissue. An irritation to the ocular surface gives rise to a large neural input, which provides the neural signal for reflex tearing. The loop is reset when the irritation is removed by copious tearing.
DRY EYE DEFINITION
The National Eye Institute defined dry eye 33 as: “a disorder of the tear film due to tear deficiency or excessive evaporation, which causes damage to the interpalpebral ocular surface and is associated with symptoms of ocular discomfort” in 1995. This definition is more clinically oriented with little emphasis on the pathogenetic mechanisms or the events that occur in response to dry eye.
During 2004-2006, International Task Force – DELPHI consensus panel on Dysfunctional tear syndrome, on the basis of pathophysiology and clinical presentation, suggested that the term dry eye does not reflect all the events occurring in the eye and hence recommended dysfunctional tear syndrome (DTS) as a more appropriate term for this disease.1,34 The term DTS has been replaced by dry eye disease (DED). Considering dry eye as a sole deficiency of one of the components of the tear film trivializes the complexity of the condition and its impact on the ocular surface health.
The Dry Eye Workshop (DEWS) in 2007 decided to improvise the definition as follows to include the pathophysiology and its impact on visual outcome, it is defined as follows , “Dry eye is a multifactorial disease of the tears and ocular surface that results in symptoms of discomfort, visual disturbance and tear film instability with potential damage to the ocular surface. It is accompanied by increased osmolarity of the tear film and inflammation of the ocular surface.”1
Lacrimal Functional Unit (LFU) 1 is an integrated system comprising of lacrimal glands, ocular surface (cornea, conjunctiva), eyelids, the meibomian and accessory lacrimal glands, and the sensory and motor nerves that connect them. This gives a more unified concept that explains the pathophysiology of ocular surface disorders. The ultimate function of this unit is to maintain the clarity of the cornea and thereby the quality of the image projected onto the retina. The definition of dry eye could therefore also be framed as: “A disorder where by dysfunction of the lacrimal functional unit causes an unstable tear film which in turn promotes ocular surface inflammation, epithelial disease and symptoms of discomfort.”
Demography35
Reported prevalence of dry eye in the literature is diverse which ranges between 7.8% in one study from western world 36 to 93.2% in one study from Asia.37
Dry eye disease in India: There are no population-based studies in relation to dry eye disease in India, however due to tropical climate and agrarian population prevalence of dry eye is high. There are only three published reports on prevalence of dry eye among hospital-based population from North and Eastern India which varies between
18.4% and 40.8%.38
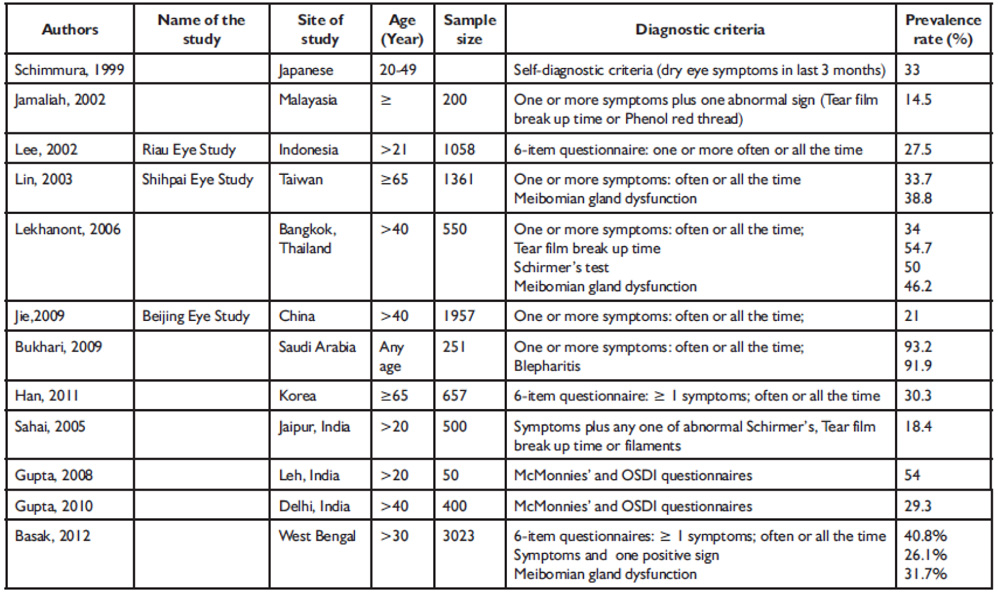
Table1: Prevalence of dry eye in different Population based studies in Asian countries
Pathophysiology 22,32
Maintaining a healthy and comfortable ocular surface requires stability and renewal of the preocular tear film. Dysfunction of any component by causing alterations in the volume, composition, distribution, and/or clearance of the tear film can lead to ocular surface disease that expresses itself as dry eye.
Two mechanisms:
1.Tear hyperosmolarity and
2.Tear film instability1
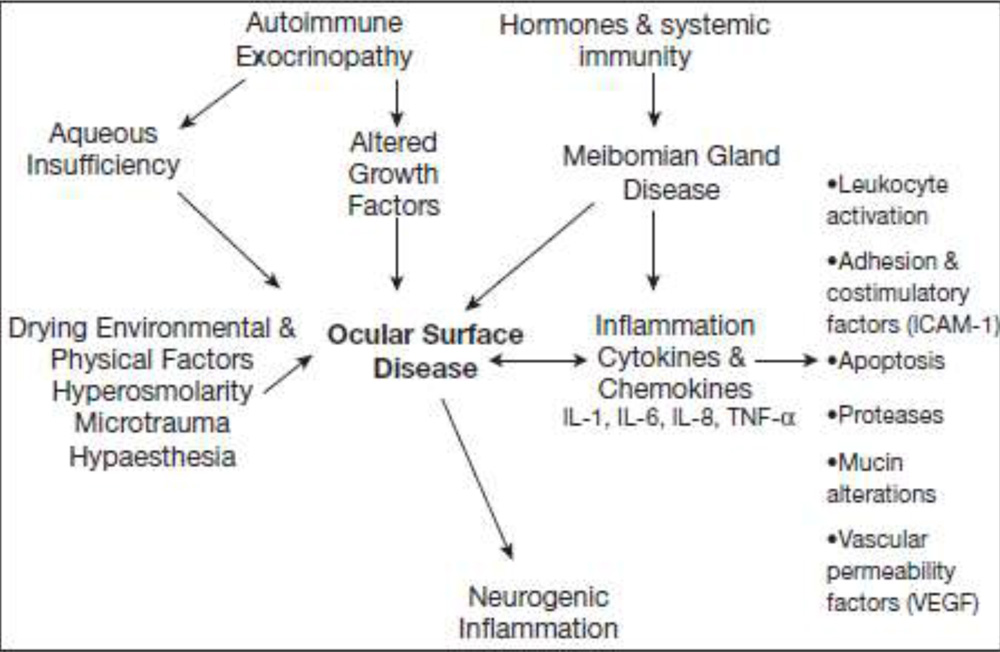
Figure 6: Pathophysiology of dry eye disorders
1.Hyperosmolarity :
Hyperosmolarity arise from either low aqueous flow or excessive tear film evaporation, or a combination. Hyperosmolar tears can damage the ocular surface epithelium by activating an inflammatory cascade in the epithelial surface cells and releasing inflammatory mediators such as the MAP kinases and NFκB signaling pathways and the generation of inflammatory cytokines (e.g., IL-1α, IL-1β, TNF-α) and MMPs, activate inflammatory cells and lead to apoptotic death of surface epithelial cells, including goblet cells and secondary lacrimal dysfunction. Tear film instability results in increased evaporation, which contributes to tear hyperosmolarity.1
2.Tear film instability:
The tear film stability is dependent on the quantity and quality of various components of the tear film, including tear viscosity, surface tension, meniscus radius, and initial and final film thicknesses. When the tear film ruptures or tear break-up appears, it may produce tear film hyperosmolality and local drying of the exposed surface, leading to the excitation of inflammatory cell markers at the ocular surface, epithelial damage and cell death by apoptosis. This may cause a disturbance of the glycocalyx and goblet cell mucins.1 These various disturbances exacerbate tear film instability, triggering a vicious cycle of events, in diagram.
Various factors contribute towards the destabilization of the tear film. Disturbances of the lipid layer result in increased evaporation of the tear film. Liotet et al suggested that the inability of the corneal epithelial cells to manufacture a glycocalyx may result in insufficient sites for mucous layer attachment, and this may be a major factor in determining tear stability.39
Van der Waals dispersion forces (attractive or repulsive forces between molecules) within the mucous layer may also cause disruption of the tear film.40 These factors independently would be inadequate to cause tear film break-up, however a combination of them will likely be adequate to cause disruption of the tear film. 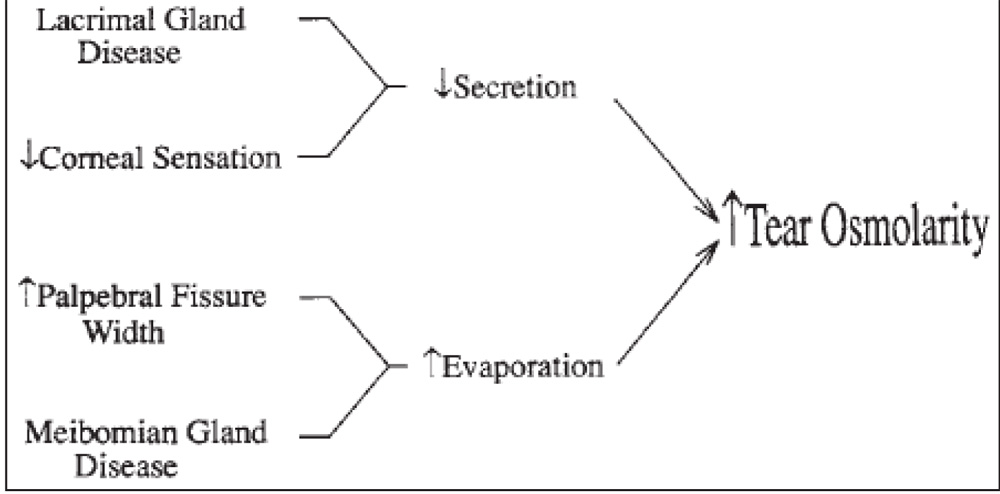
Figure 7: Mechanisms for elevated tear film osmolarity result in the surface disease.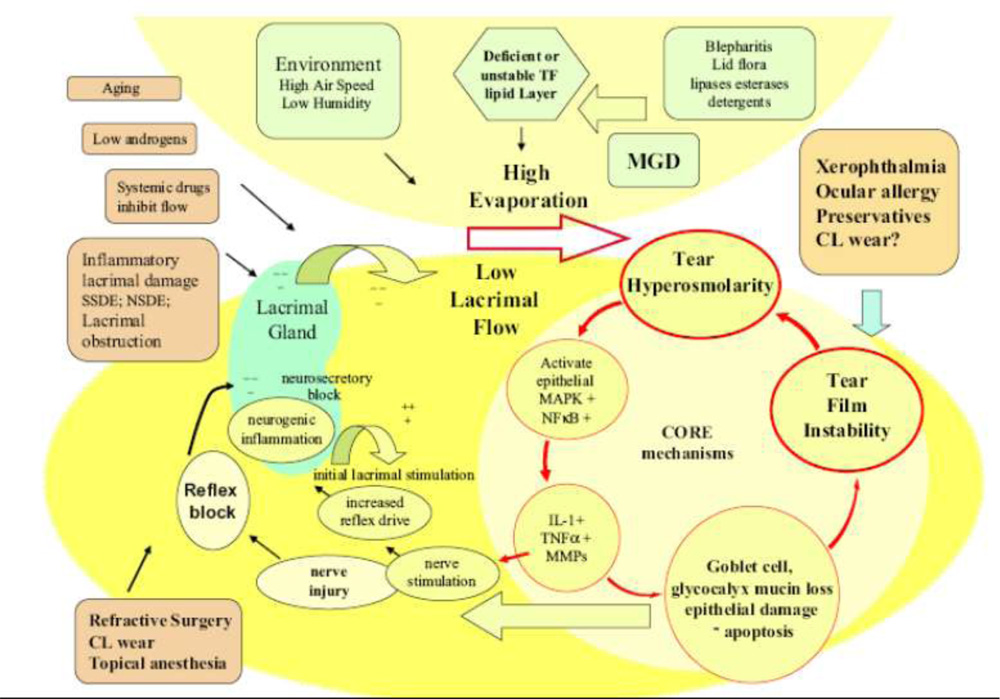
Figure 8: Mechanism for Dry Eye 1
Risk factors for dry eye
Demographic factors including age, sex and many ocular, systemic, interventional and environmental factors can be associated or cause dry eye and can also worsen an already existing condition. A diet that is deficient in Omega 3 essential fatty acid or vitamin A, medications, smoking, alcohol, and menopausal status may contribute toward the risk factors for dry eye.
1.Age, gender and sex hormones
Dry eye symptoms increase with age, especially in women and sex hormones are believed to play a role in causing dry eye.20
2.Contact lens wear
The prevalence of symptomatic dry eye in contact lens wearers occurs in 50-80% of wearers. Discontinuations and drop outs from lens wear are primarily due to symptoms of discomfort and dryness.1
3.Surgery
Dry eye can occur as a complication of laser in-situ keratomileusis (LASIK) Surgery41 and cataract surgery. Cataract surgery can effect or interrupt neurogenic response of the ocular surface and decrease tear secretion with abnormal TBUT, Oxford Scheme and Sch 1. LASIK may result in lacrimal dysfunction and decreased goblet cell density, leading to reduced tear production and an unstable tear film. 42
4.Environmental factors and computer use
An indoor working environment can cause symptoms of ocular irritation,43 particularly in those who use computers in air-conditioned workplaces, has been identified as the main environmental causative factor of dry eye.32 Low humidity, poor air quality, and pollution are other risks that may cause dry eye. 44
Effect of the environment : 32
- Milieu intérieur: Low blink rate behaviour, VTU, Microscopy, Wide lid aperture , gaze position, Ageing, Low androgen pool, Systemic drugs antihistamines, beta-blockers, antispasmodics, diuretics and some psychotropic drugs
- Milieu extérieur: Low relative humidity, High wind velocity, Occupational environment
Etiopathogenic Classification:45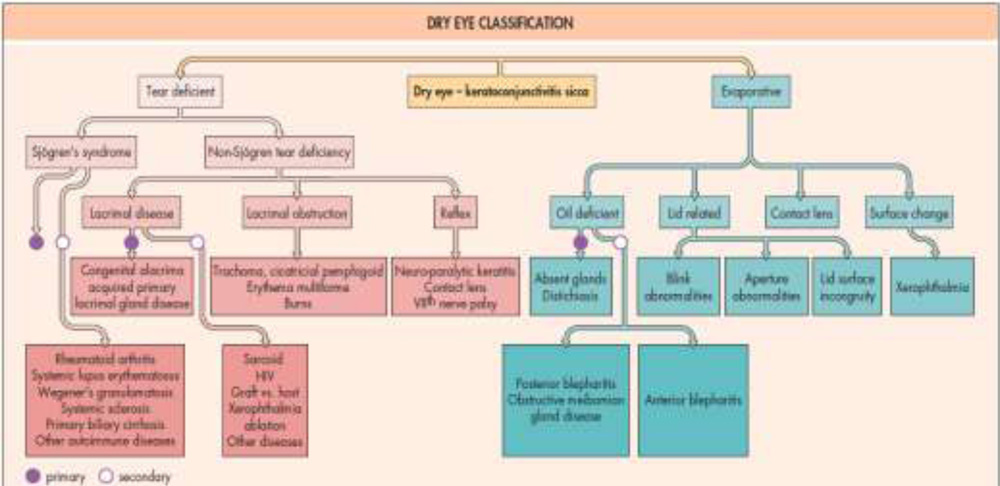
Figure 9: Dry eye classification
Aqueous tear-deficient dry eye (ADDE, tear-deficient dry eye; lacrimal tear deficiency)32
Two major subclasses:
- Sjögren’s syndrome dry eye (SSDE) and
- Non-Sjögren’s syndrome dry eye (NSSDE)
Sjögren’s syndrome dry eye (SSDE)
Sjögren’s syndrome (SS) is an exocrinopathy in which the lacrimal and salivary glands, as well as other organs, are targeted by an autoimmune process. There is a strong gender predilection for Sjögren’s syndrome, with women representing 95% of patients, with peak incidence in the fourth and fifth decades. The lacrimal and salivary glands are progressively infiltrated by activated T cells, which cause acinar and ductular cell death and hyposecretion of the tears or saliva.
There are two forms of SS 46
- Primary SS : associated systemic connective tissue disease;
- secondary SS: Consists of primary SS with autoimmune connective disease, such as rheumatoid arthritis (most common) or systemic lupus erythematosus, polyarteritis nodosa, Wegener’s granulomatosis, systemic sclerosis, primary biliary sclerosis, or mixed connective tissue disease.
Non-Sjögren’s syndrome dry eye
Non-Sjögren’s syndrome dry eye is a form of ADDE due to lacrimal dysfunction, where the systemic autoimmune features of SSDE have been excluded. This is most common form is age-related dry eye. The different forms are:
- Primary lacrimal gland deficiencies: Age-related dry eye (ARDE):
ARDE is a primary disease. lacrimal gland dysfunction is due to periductal fibrosis, interacinar fibrosis, paraductal blood vessel loss, and acinar cell atrophy.47 and decrease in androgen hormone. Androgen is required for functioning of lacrimal and meibomian gland.20
- Secondary lacrimal gland deficiencies: Lacrimal gland infiltration: Lacrimal secretion fail because of infiltration of the gland in various systemic disease like Dry eye is a common complication in graft versus host disease, and may develop in patients with systemic viral infections.1
- Obstruction of the lacrimal gland ducts
- Reflex hyposecretion :
- Sensory hyposecretion: A reduction in sensory drive from the ocular surface is thought to favour the occurrence of dry eye in two ways, first by reducing reflex-induced lacrimal secretion, and second by reducing the blink rate and hence increasing evaporative loss.41
- Diabetes mellitus: Proposed mechanisms by which diabetes mellitus may lead to dry are diabetic sensory or autonomic neuropathy, or the occurrence of microvascular changes in the lacrimal gland.48
- Neurotrophic keratitis: Extensive sensory denervation of the anterior segment, involving the cornea and the bulbar and palpebral conjunctiva, can lead to neurotrophic keratitis. This condition is characterized by features of dry eye, such as tear instability, diffuse punctate keratitis, and goblet cell loss, and also, most importantly, the occurrence of an indolent or ulcerative keratitis, which may lead to perforation.49 The sensory loss results in a reduction of lacrimal secretion and a reduction in blink rate.
- Reflex motor block: there is reduced lacrimal secretion.Responsible agents include antihistamines, beta-blockers, antispasmodics, and diuretics, and, with less certainty, tricyclic antidepressants, selective serotonin reuptake inhibitors, and other psychotropic drugs.50
Evaporative dry eye
Excessive evaporation from the exposed ocular surface has been attributed to intrinsic causes, which are due to intrinsic disease affecting lid structure or dynamics, or extrinsic causes, where ocular surface disease occurs due to some extrinsic exposure.
- Intrinsic causes
- Meibomian gland dysfunction
Meibomian gland dysfunction, or posterior blepharitis, is a condition of meibomian gland obstruction and is the most common cause of evaporative dry eye.51 It can be both the starting cause and the downstream consequence of dry eye disease.
- Disorders of lid aperture and lid/globe congruity or dynamic
An increase in the exposed evaporative surface of the eye occurs in craniostenosis, endocrine (e.g., thyroid) and other forms of proptosis. Lagophthalmos, especially nocturnal, is also a common cause of increase evaporative surface.
- Low blink rate
Drying of the ocular surface may be caused by a reduced blink rate, which lengthens the period during which the ocular surface is exposed to water loss before the next blink. This may occur as a physiological phenomenon during the performance of certain tasks requiring concentration, e.g., chronic viewing of a video screen or microscope, or it may be a feature of an extra pyramidal disorder, such as Parkinson’s disease.
- Extrinsic causes
- Ocular surface disease
Disease of the exposed ocular surface may lead to imperfect surface wetting, early tear film breakup, tear hyperosmolarity, and dry eye. This can occur in any chronic surface disease, such as allergic conjunctivitis, or in nutritional causes such as vitamin A deficiency.
Topical drops can also cause ocular surface toxicity and secondary tear film disruption. The most common etiologic agent is benzalkonium chloride (BAC), which causes surface epithelial cell damage and punctate epithelial keratitis, which interferes with surface wettability.1
- Contact lens wear
Pre-lens tear film thinning time together with poor lens wettability, could be a basis for a higher evaporative loss during lens wear and was attributed to potential changes in tear film lipid composition , rather than to a loss of meibomian gland oil delivery.
Symptoms: 52
Presenting complaints: Irritation, tearing, burning, stinging, dry or foreign body sensation, mild itching, photophobia, blurry vision, contact lens intolerance, redness, mucous discharge, increased frequency of blinking, diurnal fluctuation, and symptoms that worsen later in the day.
Exacerbating conditions: Wind, air travel, decreased humidity, prolonged visual efforts associated with decreased blink rate such as reading or watching TV.
TEAR FILM EVALUATION 22,32,45
1) GENERAL INSPECTION
- Gross examination of the ocular adnexa can reveal significant structural changes important in the pathogenesis of dry eye disease. The eyelid structure and function can be examined with bright natural or artificial light.
- Normally eyelids should approximate the ocular surface and the upper lid should travel over two-thirds of the cornea with each blink.
2)SLIT LAMP EXAMINATION
- Tear Volume Assessment
Examination of the inferior marginal tear strip can yield information about the volume of tears present on the ocular surface. The tear strip is a line of tears just above the lower lid. It is normally about 0.5 mm in width and has a concave upper aspect. When this strip is thin or discontinuous, it is evidence of deficient aqueous tear volume (late sign). It is normally seen under slit lamp and measured by reflective meniscometry,53 or by assessing its profile photographically in slit section.54
Other non invasive method are: Optical coherence tomography, Strip meniscometry , Tearscope Plus using interference phenomena.
3)EVALUATION OF TEAR FILM STABILITY
Tear film breakup time:
It is the interval b/w the last blink and the appearance of the first randomly distributed dry spot.55 It is abnormal in aqueous tear deficiency, meibomian gland disorder and evaporative dry eye. 2% fluorescein is instilled in lower fornix, and patient is asked to blink several times. Tear film is examined at the slit lamp with a broad beam using the cobalt blue filter. After an interval, usually 10–30 seconds the tear film thins, leading to the development of randomly distributed dry spots in the precorneal tear film. Values of less than 10 seconds are considered abnormal.56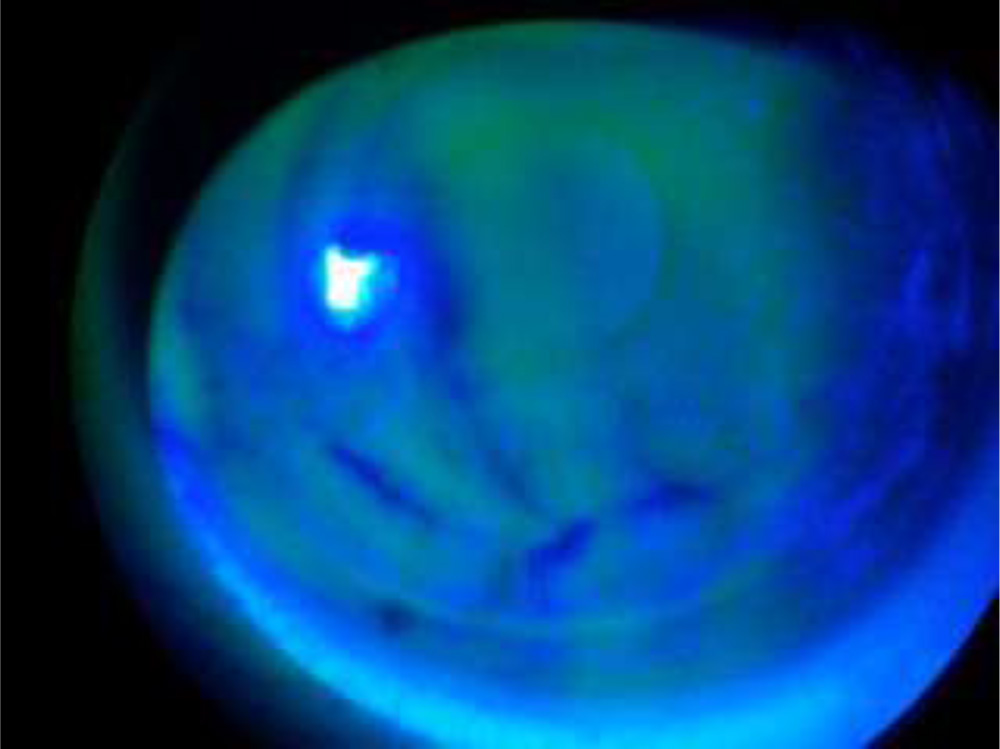
Figure 10: Tear Break Up
Ocular Protection Index (OPI):
OPI = TBUT / IBI (Inter-blink interval).
- OPI <1.0 : characteristic of tear film instability and dry eye disease.
- OPI ≥1.0 : Normal
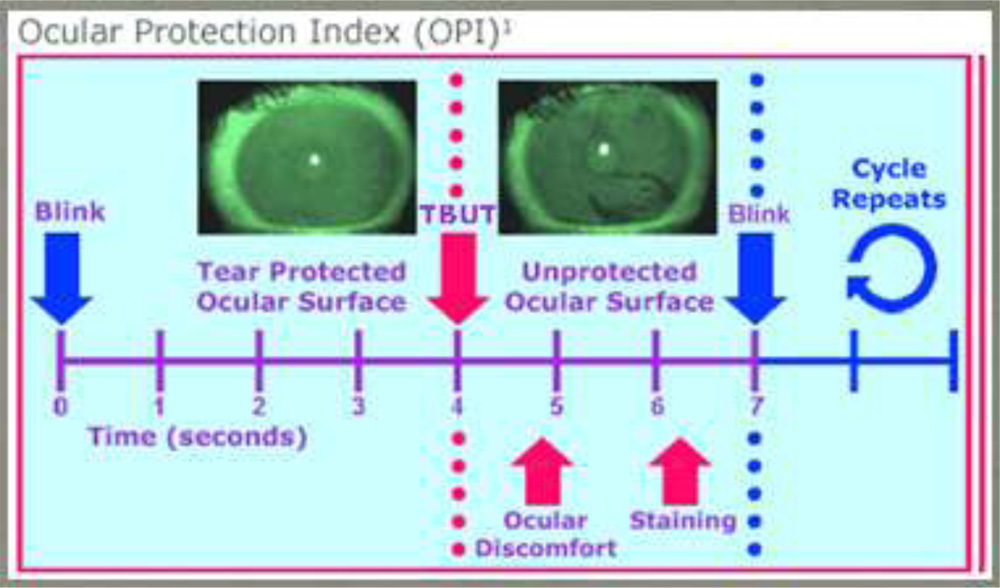
Figure 11: Ocular Protection Index
NON INVASIVE TBUT:
- Non-invasive tear break-up time (NIBUT) involves the observation of an illuminated grid pattern reflected from the anterior tear surface.
- NIBUT can be measured by:
a) Corneal topography
b) Interferometry
c) Aberrometry
d) Functional visual acuity assessment
- Corneal topography
- Uses:
- tear film stability
- evaluate corneal surface regularity
- evaluation of post LASIK dry eye
- Uses:

Figure 12: Tear Film Topographer
Lipiview interferometry
- Coloured fringes that arise from interference between light reflected from the surface of the lipid layer and from the interface between the lipid layer and the aqueous layer of the tear film
- Used to observe the nature, thickness and rupture of the lipid layer

;Figure 13: Lipiview Interferometer
- Wave front aberrometer
- Visual disturbances caused by higher order aberrations arising from tear film instability and break-up is assessed
- Aberrometry is also used for monitoring the efficacy of treatments
4)TEAR SECRETION ASSESSMENT
1.Schirmer’s test – Originally described in 190322 for tear quantity. This is the most widely used test to measure aqueous tear production. In this test a standardized size strip of filter paper i.e. Whartmann-41 paper 5mm x 35mm is inserted over the lower lid margin into the cul-de-sac, usually in the temporal one-third of the lid for 5 minutes.32
Type –I (without anaesthesia)
- Basal And Reflex Secretion
Van Bijsterveld selected a cut off 5.5mm strip wetting in 5 min.57 Normal results are often greater than 10 mm; results of 5 mm or less for the Schirmer test without anesthesia are generally considered abnormal and serially consistent results are highly suggestive.22
Figure 14: Schirmer’s Test
Type-II (with anaesthesia)
- basal secretion of tears58
Though it has been purported to measure ‘basal’ tear secretion, i.e. non stimulated tears. It has been demonstrated that, even with anaesthesia of the cornea and conjunctiva, tear secretion is driven by sensory stimuli, of the lids, lashes, air currents, and light.
These tests has been criticized for its variability as differences in performance of the test will greatly influence the sensory stimuli. The Schirmer’s test, however, is a useful estimate of aqueous tear production because of its ease of performance, wide availability, and low cost.
Type III-
reflex secretion
Phenol Red Test59: This involves the use of a special cotton thread that has been impregnated with a dye – phenol red. The thread is inserted over the inferior lid margin into the temporal conjunctival sac. At the end of 15 seconds, the dye, which is pH sensitive, turns color from yellow to orange, indicating the length of the thread wetted by tears. This test has been reported to be less uncomfortable and more specific in the diagnosis of aqueous tear-deficient dry eye disease.
5.OCULAR SURFACE DAMAGE ASSESSMENT
The normal ocular surface does not take up water-soluble dyes instilled into the tear film. With disruption of the mucin coating protecting the surface epithelial cells and/or damage to the epithelial cell walls, water-soluble dyes will diffuse into the surface cells.
The three most commonly used dyes are fluorescein, Rose Bengal (RB), and lissamine green (LG). The red-free filter makes examination easier.
LG stains degenerated cells, dead cells and mucous fibrils in the same manner as RB. LG is preferred more than RB staining as it is equally effective and causes less irritation, pain and itching. It is neither carcinogen nor toxic. The surface of the conjunctiva can be viewed within 10 seconds with RB and 2–3 minutes after LG stain, and low light should be used.
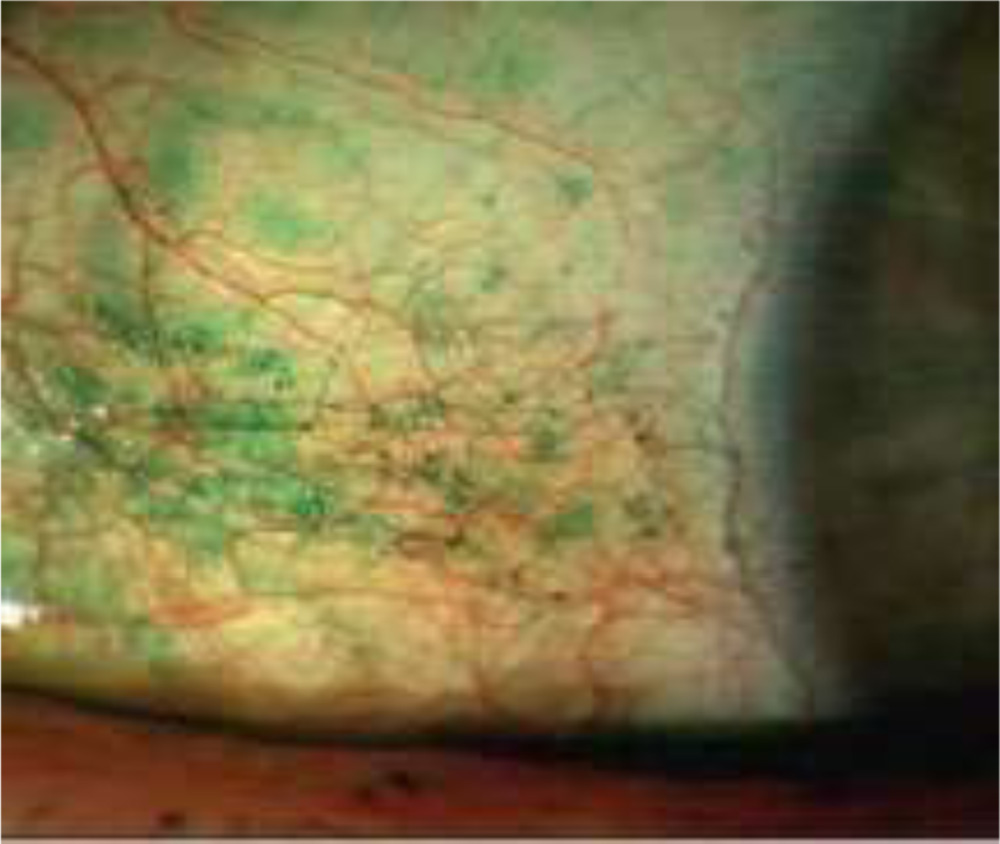
Figure 15: Lissamine Green Staining
Fluorescein is a yellow water soluble di-basic acid dye of Zanthine Series that produces intense green fluorescent colour in alkaline solution. Chmically it is C2H12O5NA.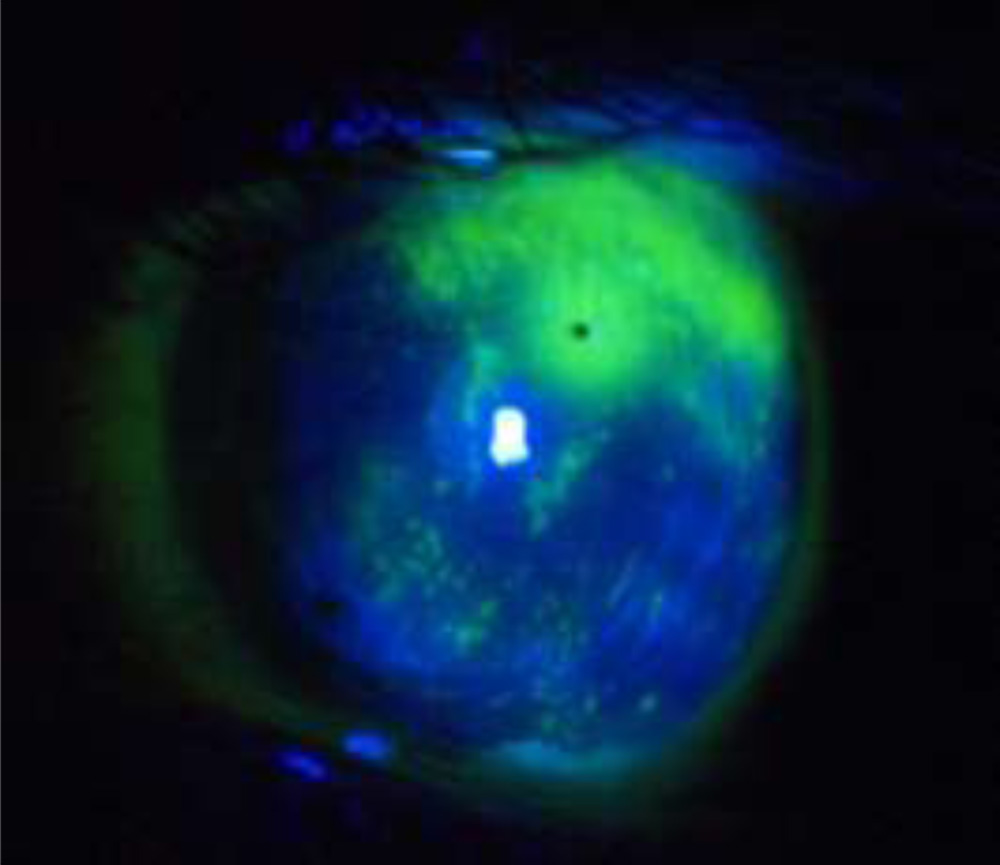
Figure 16: Fluorescein Staining
There are a number of grading scales, including the Van Bjisterveld, NEI/Industry Workshop, and Oxford systems.60
a) Van Bijsterveld developed a scoring system for RB dye that divides the ocular surface into three zones: nasal bulbar conjunctiva, cornea, and temporal bulbar conjunctiva.(14) Each zone is given a score ranging from zero to 3, with zero indicating no staining and 3indicating essentially confluent staining.
b) Oxford scheme grades the conjunctiva and cornea together using fluorescein and rose-bengal or lissamine green stain. It was developed to quantify epithelial damage in case of dry eye, uses a chart with a series of panels labeled A-E in order of severity (absent, minimal, mild, moderate, severe).61
c)The NEI workshop grading system:It uses fluorescein to grade the cornea and rose-bengal for conjunctiva. A score of > 3 out of 15 and >3 out of 18 is considered abnormal for the cornea and conjunctiva respectively.
6) TEAR CLEARANCE ASSESSMENT
Tear turnover is defined as the rate at which newly secreted tears reside within the tear film before its lost due to evaporation or drainage through the lacrimal punctae and the nasolacrimal ducts. Tear volume and turnover are measured by dye dilution studies. In this methodology, a small amount of fluorescein dye is instilled into the tear film and the concentration of the dye is measured over time by fluorophotometers.
Alternative and inexpensive method (Fluorescein Clearance Test [FTC]), 5 μL of 1% fluorescein dye is instilled into the tear film. The patient is asked to blink to distribute the dye and serial 1-minute Schirmer’s tests are performed every 10 minutes. Initially, the staining is intense. Persistent staining (beyond 10 minutes) indicates delayed tear clearance (DTC).
Tear function index (TFI) is the ratio of the value of the Schirmer’s test over the tear clearance rate.62
7) ASSESSMENT OF TEAR COMPOSITION AND CHARACTERISTIC
Qualitative and quantitative techniques to assess major aqueous components (proteins) include one-and two-dimensional polyacrylamide gel electrophoresis (PAGE), isoelectric focusing (IEF), crossed immunoelectrophoresis, enzyme-linked immunosorbent assay (ELISA), and high-pressure liquid chromatography (HPLC) techniques such as size-exclusion HPLC, reversed-phase HPLC, and ion-exchange HPLC. Matrix-assisted laser desorption/ionization (MALDI) mass spectrometry has also been applied to study changes in tear proteins before and after corneal wound healing, and proteomic methods have been used to map tear protein profiles.
Tear ferning:
Tear samples are dried on a slide and examined under a microscope display a crystalline pattern of tear mucin. In aqueous tear deficiency, this pattern resembles ferns.
Classified into 4 groups:
a) Uniform arborisation and numerous branching are seen. little or no space between ferns.
b) Branching is less and there is abundant space between ferns.
c) Ferns are thicker and smaller with little branching and very large spaces between them.
d) No ferning but amorphous pattern is seen.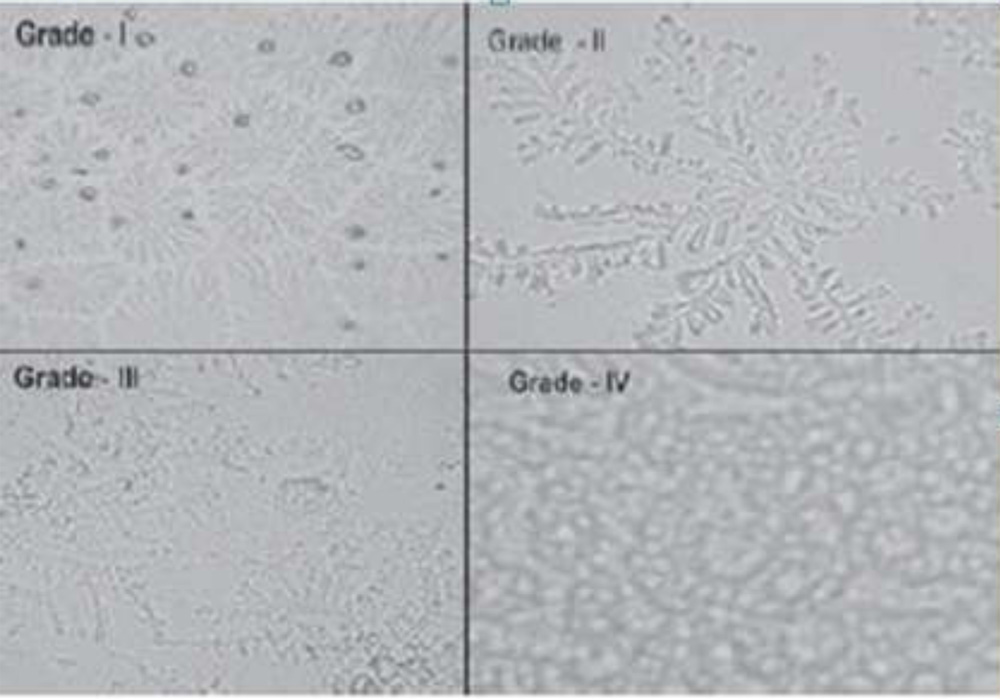
Figure 17: Ferning patterns classification
Tear osmolarity:
Tear film osmolarity has been measured using freezing point depression and vapor pressure measurement. A recent report suggests very high sensitivity and specificity and positive predictive values for this TearLab technology, making this a new ‘gold standard’ in the diagnosis of dry eye disease.63
Dry eye disease the tear film is in a hyperosmolar state. This is true for both aqueous deficient and evaporative dry eye disease
Conjunctival impression cytology:
It is a substitute for conjunctival biopsy.
Severity of dry eye :
Stage 0: normal cellular structure
Stage 1: early loss of goblet cells without keratinisation
Stage 2: total loss of goblet cells with slight enlargement of epithelial cells
Stage 3: early and mild keratinisation
Stage 4: moderate keratinisation
Stage 5: advanced keratinisation
8) TESTS OF VISUAL FUNCTION
Recent, attention is directed to optical aberrations which is identified in patients with dry eye disease. The instability which is characteristic in all forms of dry eye disease results in rapid break-up of the tear film between blinks, compromising image quality. This effect on visual acuity is not captured during ordinary Snellen because the patient can blink, momentarily improving vision. More rapid break-up occurs within 3 second of a blink in many dry eye patients, reducing their inter-blink acuity to levels of 20/60 or less.64 The two instrument is developed to detect these changes. In one, the tear stability analysis system, serial videokeratographic images are collected each second between blinks. In another, a functional visual acuity device has been developed which measures visual acuity by way of rapid presentation of optotypes. Both of these technologies are important in diagnostic technologies in the near future.
9) MEIBOMIAN GLAND STRUCTURE AND EXCRETA
(i) Slit lamp inspection of the lid margin and estimate the quantity and quality of the excreted lipid (meibum). Evidence of altered meibomian gland structure includes increased vascularity of the lid margin, plugging of the orifices, and loss of orifices.65
(ii) Evaluate by pressing against the lower lid with a finger about 1 mm below the lid margin, excretion is normally fluid and clear. Lack of expression and/or alteration in the character of the excretion, is critical in the diagnosis of meibomian gland dysfunction (MGD). As the disease process, the excretion will vary from turbid to coagulated (toothpaste-like). Such meibum is pathognomonic of MGD.
(iii)Transillumination of the eyelid. Using an examining muscle light placed inside the lower eyelid (after topical anesthesia), it is possible to visualize the outline of the glandular structure. This visualization can be enhanced and recorded with the use of infrared film.
10) CORNEAL SENSITIVITY
Reduced corneal sensation can be both the cause and the effect of dry eye. Sensory denervation may lead to dry eye by several mechanisms:
(1) reducing the afferent signal that drives aqueous tear secretion,
(2) reducing the blink rate (leading to ocular surface desiccation), and
(3) altering the growth and differentiation of ocular surface epithelia through diminished trophic influences of the trigeminal nerve
This reflects global dysfunctioning of the ocular surface lacrimal gland functional unit and secondary decreased neural sensitivity. Macri and Pflugfelder66 have used a Cochet-Bonnet esthesiometer, uses a monofilament nylon which is extendable from 0-60 mm. When applied perpendicularly to the corneal surface with a bending angle of 5 degrees, this thread exerts pressures from 11-200 mg/mm2 correlating inversely with the length of the filament. In routine clinical practice, a cotton wick can be used to assess the presence, or absence of corneal sensation.
11) NFLAMMADRY
- Measures Metalloproteinase-9, a non-specific marker of inflammation ,by taking swab from the fornices. It is non-specific to dry eye but highly correlated
MANAGEMENT OF DRY EYES 22,32
The main objectives in caring for patients with dry eye disease are to improve their ocular comfort and quality of life, and to return the ocular surface and tear film to the normal homeostatic state.
Patient education about the natural history and chronicity of the dry-eye disorder is crucial to successful management of this Condition.
- Avoidance of Exacerbating Factors
Environmental modifications such as humidification, avoidance of wind or drafts and avoidance of dusty or smoky environments may ameliorate dry eye symptoms.
- Warm Compresses and Lid Hygiene 22
Warm compresses are indicated in patients with meibomitis or meibomian gland dysfunction. The patent is instructed to place a clean washcloth under hot water and then apply it to closed lids while massaging both upper and lower lids with their fingertips. The massaging action combined with heat helps express lipid into the tear film, preventing retention of lipid within the meibomian gland which may be a stimulus for inflammation. Lid hygiene consists of cleansing the crust and scurf from the eye lashes with baby shampoo.
- Dietary modifications to avoid dry eyes
Vitamin A:cod liver oil, liver, carrots, sweet potatoes, butternut squash.
Lutein and zeaxanthin:spinach, kale, collard greens.
Vitamin C:strawberries, broccoli, oranges,
Bioflavonoids:citrus fruits, cherries, grapes, plums.
Vitamin E:sunflower seeds, almonds, hazelnuts.
Selenium:brazil nuts, yeast, seafood.
Zinc:oysters, hamburgers, wheat, nuts
Fatty acids:cold-water fish
- Tear Supplementation22,32
Lubricants, including artificial tears, ointments, and gels, are still the mainstay of therapy in all stages of DED, either alone (in mild to moderate disease), or in combination with other treatments (in moderate to severe disease).67
Role of tear supplements:
act as lubricants;
replacement of deficient tear constituents,
dilute pro inflammatory substances,
reduces tear osmolarity1,67 and
protect against osmotic stress.1
Ocular lubricants are characterized by hypotonic or isotonic buffered solutions containing electrolytes, surfactants, and various types of viscosity agent. The ideal artificial lubricant should be preservative free. The electrolytes particularly contains potassium and bicarbonate, and have a polymeric system to increase its retention time. Physical properties include a neutral to slightly alkaline pH. Osmolarities of artificial tears have been measured to range from about 181 to 354 mmol/L.1
Artificial tears contains compatible solutes which are small non ionic molecules (e.g., glycerin) causing increased intracellular osmolarity and thus provides protection against osmotic stress.
Colloid osmolality (which relates to macromolecule concentration) influences water transport across the ocular surface epithelium. It also reduces swelling of damaged epithelial cells.1
It act as viscosity agents. The viscosity agent increases residence time and slows the rate of clearance. It also protect the ocular surface epithelium by either coating and protecting it by restoring the protective effect of mucins, thus reduces frictional stress.68 Viscosity agents used in artificial tears include carboxymethylcellulose, polyvinyl alcohol, polyethylene glycol, propylene glycol, hydroxypropyl-guar (HP-guar), and lipids such as those that make up castor oil or mineral oil.1
Ocular ointments and gels are also used in treatment of dry eye disease. Ointments are formulated with a specific mixture of mineral oil and petrolatum. In general, ointments do not support bacterial growth and therefore do not require preservatives. Ophthalmic gels and ointments have higher viscosity and thus a longer contact time than liquids.
Anti-inflammatory therapy32
As inflammation is a key component of the pathogenesis of dry eye. Inflammation can be due to hyperosmolarity, chronic irritative stress (e.g., contact lenses), and systemic inflammatory / autoimmune disease (e.g., rheumatoid arthritis).
Ciclosporin A (CsA): It is a fungal-derived peptide, a calcineurin inhibitor. It is currently the only pharmacologic treatment that is FDA approved specifically for DED.
- In studies of DED patients, ciclosporin reduces:
- proinflammatory cytokines (e.g., conjunctival IL-6 levels),
- activated lymphocytes in the conjunctiva,
- conjunctival inflammatory and apoptotic markers, and
- increases conjunctival goblet cell numbers
- Adverse effects are ocular burning and stinging sensation.
Corticosteroids: It exert their immunosuppressive effects by non specifically inhibiting many aspects of the inflammatory response. Their immunomodulatory actions are due to inhibition of the activity of transcription factors such as activator protein-1 (AP-1) and nuclear factor κB (NFκB).
Tetracyclines: The clinical benefits in DED are most likely due to their antibacterial, anti-inflammatory and protease inhibitory properties. Tetracycline derivatives (e.g., minocycline, doxycycline) are generally preferred to tetracycline because of their high concentration in tissues, low renal clearance, long half-life, high level of binding to serum proteins, and decreased risk of photosensitization.1
- Tear stimulation: secretagogues
Several potential topical pharmacologic agents may stimulate aqueous secretion, mucus secretion, or both. Among several agents which are currently under investigation by pharmaceutical companies, the safety and efficacy of diquafosol (one of the P2Y2 receptor agonists) eye drops has been favourably evaluated in several experiment.69 Orally administered cholinergic agonists, in particular pilocarpine and cevilemine, are sometimes given to treat severe aqueous-deficient DED.
- Biological tear substitutes
1.Serum
Autologous serum tears, produced from the patient’s serum, have been used in severe DED. The protocol used for the production of serum eye drops determines their composition and efficacy. The tears are typically unpreserved, but can be stored frozen for 3–6 months.1 The reports of successful treatment of persistent epithelial defects is noted.
Generally, autologous serum drops shows marked suppression of apoptosis in the conjunctival and corneal epithelium. Albumin, the major protein in serum, improves ocular surface damage in vivo and rescued apoptosis after serum deprivation in vitro.70 Few complications reported with autologous serum tears; are discomfort, slight epitheliopathy, bacterial conjunctivitis or eyelid eczema.71
1.Autologous platelet rich plasma: Platelet-rich plasma contains high numbers of platelets that produce growth factors. The induce mesenchymal and epithelial cells to migrate and proliferate. Platelet-rich plasma has a lubricating effect.72
2.Salivary gland auto transplantation: Salivary submandibular gland transplantation is capable of replacing deficient mucin and the aqueous tear film phase. surgery is capable of substantially reducing discomfort, but often has no effect on vision. Patients with absolute aqueous tear deficiency, viable submandibular gland grafts provide significant improvement in the Schirmer test, TBUT, and rose Bengal staining, as well as reduction of discomfort and the need for pharmaceutical tear substitutes. Owing to the hypo-osmolarity of saliva compared to tears, excessive salivary tearing can induce a microcystic corneal edema, which is temporary but can lead to epithelial defects.1 Hence, this operation is indicated only in end-stage DED.
- Tear retention
Punctal occlusion is one of the most useful and practical therapies for conserving tears in patients with aqueous-deficient DED.1 Punctal and intracanalicular plugs generally provide a temporary and reversible means of occlusion, and electrocautery or laser are used for more permanent punctal occlusion. The argon laser is used to achieve the desired level of punctal stenosis based on the patient’s tear function. The wide choice of reversible devices currently available has reduced the need for occlusive surgery. The punctal plugs are divided into two main types: absorbable and non absorbable. The former are made of collagen or polymers and last for variable periods (3 days to 6 months). Some newer absorbable materials may last as long as 6 months. The non absorbable ‘permanent’plugs include the Freeman style, which consists of a surface collar resting on the punctal opening, a neck, and a wider base, and are made of silicone or hydrophilic acrylic. Contraindicated in dry eye patients with clinical ocular surface inflammation. A common complication of punctal plugs is epiphora, spontaneous plug extrusion, which is particularly common with the Freeman-style plugs, internal migration of a plug, biofilm formation and infection,1 and pyogenic granuloma formation.
granuloma formation.
1.Moisture chamber spectacles: They reduce tear evaporation by increasing humidity around the eye. The patient’s glasses can be modified using commercially available top and side shields, or for more severe cases swimming goggles can be used.
2.Contact lenses: They are used in severe dry eye or when other therapies have failed, to help retain the tear film and/ or promote ocular surface healing.
- Low water content HEMA lenses are for moderate dry eyes.
- Silicone rubber lenses are no water content and transmits oxygen very effective in protecting cornea in extreme tear film deficiency, although deposition of debris on surface of lens may blur the vision.
Occlusive gas permeable lenses: provides a reservoir of saline over the cornea
Tarsorrhaphy: It is done to narrow the palpebral aperture,decreasing evaporation by reducing the area of exposed ocular surface for patients who have developed severe epitheliopathy, persistent epithelial defects, or frank stromal ulceration. If partial closure fails, complete closure may be indicated.
Vitamin A deficiency is a known cause of xerophthalmia; however, most DED patients are not vitamin A deficient. Limited data suggests that a possible role of vitamin A in reversing conjunctival squamous metaplasia and keratinization in severe DED.
- Mucolytics
Topical acetylcysteine was mentioned in the literature as a DED treatment as early and is still sometimes used in patients with dense mucus accumulation or filamentary keratitis.
- Botulinum toxins
It may be required to induce ptosis to decrease tear evaporation in patients with severe dry eye Repeat injection may require in many situations.73
 Meibomian gland probingTopical Vitamin A (retinol)
Meibomian gland probingTopical Vitamin A (retinol)
Figure 18: Meibomian gland probe
Indications:Swollen tender lids, symptomatic MGD
Disposable probes 1mm-6mm probes. Can deliver steroids through probe
Must continue MGD Rx: Doxycycline, Omega 3 etc
- LipiFlow :
Rests on the sclera without touching the cornea. Heat and pressure are directed at the meibum, effectively massaging the structures to soften and release the obstruction that characterizes meibomian gland dysfunction. The treatment works by increasing blood flow around the meibomian gland, thus facilitating heat transfer, and, secondly, by mechanically removing blockage in the passages. Disadvantage: The device and the disposable eye cups for each patient is very expensive.
TREATMENT GUIDELINES
Previous practice guidelines have used an etiology-oriented approach to DED.1 However, commonly used etiologic classifications (e.g., aqueous-deficient vs evaporative, Sjögren’s vs non-Sjögren’s) often are not helpful in establishing a treatment plan.34
International Task Force guidelines, published in 2006, propose a classification of DED severity based on clinical signs and symptoms. In 2007 the Management and Therapy Subcommittee of the International Dry Eye WorkShop (DEWS) adopted a modified form of the ITF severity grading, as shown in Table 2.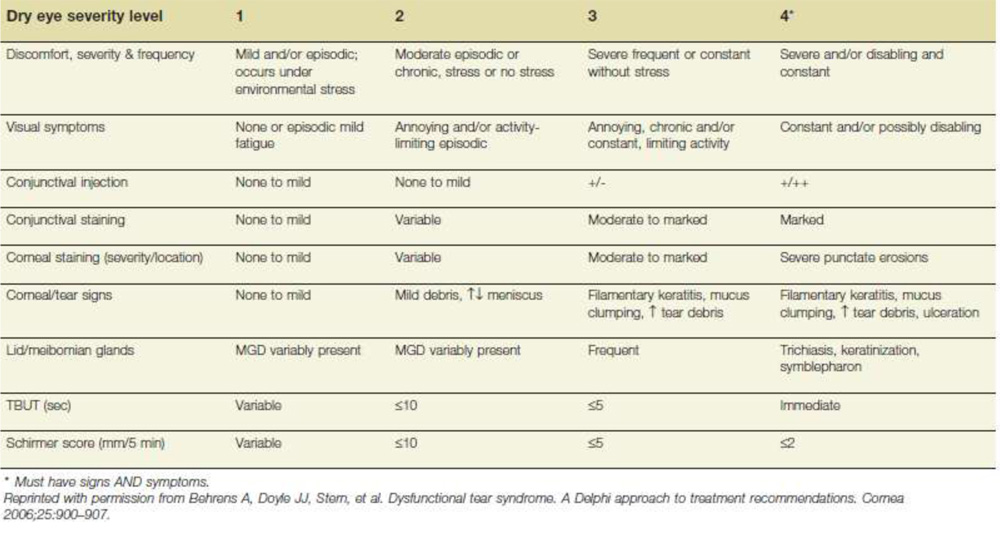
Table 2: Treatment Recommendations for Dry Eye Disease by Disease Severity Level1
The DEWS treatment recommendations are based on the modified severity grading.
- Severity Grade Treatment Recommendations 1
- Mild
Education and Environment modifications
Elimination of offending topical and/or systemic medications
Aqueous enhancement: Artificial tear substitutes; gels/ ointments
Eyelid therapy (warm compress and eyelid hygiene)
Treatment for contributing ocular factors such as
Blepharitis or meibomianitis.e.g.,Systemic Tetracyclines
- Moderate
In addition to above treatments:
Anti-inflammatory agents (topical cyclosporine and
corticosteroids), systemic Omega-3 fatty acids supplements
Punctal plugs
Spectacle side Shields; Moisture chamber goggles
- Other
In addition to above treatments:
Systemic cholinergic agonists; Oral pilocarpine. cevimeline
Systemic anti-inflammatory agenis
Mucolytic agents
Autologous serum tears
Contact lenses
Permanent punctal occlusion
Repair of eyelid abnormalities (malpositions or exposure)
Tarsorrhaphy
Mucus membrane, amniotic membrane transplantation
- Ongoing clinical trials 74
Thymosin Beta 4 (TB 4)
Thymosin Beta 4 is a synthetic copy of the naturally occuring 43- amino acid peptides. It promotes would repair and regeneration in various tissues. In the eye, it promotes corneal epithelial cell migration, decreases cell inflammation and has anti apoptotic activities. It upregulates the gene expression of laminin 5 , a major sub epithelial adhesion protein located in basement membrane of cornea and conjunctiva and is important in wound healing.
Hodroxy Propyl Guar Galactomannan
- Studies have shown the efficacy of 0.25% (HPGG) ophthalmic gel for the treatment of dry eye by showing mean change from base line in fluorescein staining score and symptom questionnaire score.
Lotemax
Lotemax, an ophthalmic cortico steroid, targets inflammation with unique site active mechanism of action. Structural modification makes lotemax highly lipid soluble, enhancing penetration into the cells and exert anti-inflammatory activity within the eye. Anti inflammatory activity of lotemax may help mitigate the stinging with cyclosporene administration and dry eye signs and symptoms experienced during the initiation of therapy. Restasis is indicated to increase tear production in patients whose tear production is presumed to be supressed due to occular inflammation
Dexamethasone Phosphate (Ocular lontophoresis)
EGP -437 at two different dose levels: Ocular lontophoresis with EGP-437 4.0 mA-min at 1.5 mA and Ocular lontophoresis with EGP-437 6.5 mA-min at 2.5 mA compared to Ocular lontophoresis with placebo (sodium citrate buffer solution) for treatment of sign and symptoms of dry eye is evaluated.
MATERIALS AND METHODS
STUDY DESIGN
Comparative hospital based study
STUDY SETTING
The Department of Ophthalmology, Kempegowda Institute of Medical Sciences & Research, Bangalore
MATERIALS AND METHODS
After obtaining the institutional ethics committee approval, 150 patients, who consented to be included in the study, of either sex, undergoing small incision cataract surgery with and without diabetes admitted at ophthalmology department, KIMS hospital, Bangalore from Dec. 2013 to May 2015 were included in the study.
Study duration:
- One and a half year
Sample size:
- A total of 150 eyes of 150 patients undergoing SICS at KIMS, of which 75 having diabetes and 75 control group without diabetes.
Inclusion criteria:
- Patients above 40 years of age, undergoing SICS at KIMS hospital during study period were selected.
- Age and sex matched diabetic and non diabetic patients were selected as study group and control (75 each).
- Consenting patients were included.
Exclusion criteria:
- Previous ocular surgeries.
- Pre existing ocular surface disease and lid abnormality.
- Previous long standing drug therapy (tropical or systemic steroids)
- Autoimmune diseases.
- Smoker.
- Pre existing ocular disease
Glaucoma
Uveitis
Ocular allergy
Pterygium
Blepharitis.
- Patients disagreeing to give informed consent
Patient admitted were selected on the basis of inclusion and exclusion criteria. Demographic details like name, age, sex, occupation, address and IP no. was documented.
- Pre operative evaluation
Detailed medical history and examination done along with investigations like Complete blood count, FBS, PPBS, HBsAg, HIV, HbA1C , blood urea and Serum Creatinine(as required), ECG.
Ophthalmic examination: Visual acuity using Snellen’s chart , detailed slit lamp examination of the anterior segment and grading of cataract, posterior segment evaluation using indirect ophthalmoscope, Intra ocular pressure measured using rebound tonometer, external view of the eye, noting lid structure, position, symmetry, and blink dynamics

Fig 20: Slit Lamp Examination
Ocular symptoms of dry eye was graded according to the level of severity characterized by burning, stinging, redness, sensation of a foreign body as per following table
| Symptom Score | Remarks |
| 0 | Absent |
| 1 | Mild |
| 2 | Moderate |
| 3 | Severe |
| 4 | Very severe |
- Biomicroscopic examination of the tear film75
- Tear break up time (TBUT)
| Value (in Sec.) | Remarks |
| >10 | Normal |
| ≤10 | Abnormal |
- Schirmer1
| Value (in mm) | Remarks |
| >10 | Normal |
| ≤10 | Abnormal |
- Tear meniscus height
| Value (in mm) | Remarks |
| <.5 | Abnormal |
| ≥ .5 | Normal |
Biomicroscopic examination of the corneal and conjunctival staining was done using Lissamine green (LG) and Sodium fluorescein (SF) respectively which was graded according to Oxford scheme grading. Order of severity labeled as follows
| Label | Severity |
| – | Absent |
| + | Minimal |
| ++ | Mild |
| +++ | Moderate |
| ++++ | Severe |
Biomicroscopic examination of the lid margins and meibomian gland orifices.
- All above tear film evaluation was done post operatively during following period: 1st week, 3rd week and 6th week
- The data collected were recorded as per each visit and subjected to statistical analysis.
Statistical Methods76-79:
Descriptive and inferential statistical analysis has been carried out in the present study. Results on continuous measurements are presented on Mean ± SD (Min-Max) and results on categorical measurements are presented in Number (%). Significance is assessed at 5 % level of significance. The following assumptions on data is made:
Assumptions:
1.Dependent variables should be normally distributed,
2.Samples drawn from the population should be random, Cases of the samples should be independent
Student t test ( two tailed, independent) has been used to find the significance of study parameters on continuous scale between two groups (Inter group analysis) on metric parameters.
Chi-square/ Fisher Exact test has been used to find the significance of study parameters on categorical scale between two or more groups.
Significant figures :
+ Suggestive significance (P value: 0.05<P<0.10)
* Moderately significant ( P value:0.01<P £ 0.05)
** Strongly significant (P value : P£0.01)
Statistical software: The Statistical software namely SAS 9.2, SPSS 15.0, Stata 10.1, MedCalc 9.0.1 ,Systat 12.0 and R environment ver.2.11.1 were used for the analysis of the data and Microsoft word and Excel have been used to generate graphs, tables etc.
RESULTS
Study design: Comparative hospital based study conducted on 150 eyes of 150 patients of either sex, undergoing small incision cataract surgery with and without diabetes admitted at ophthalmology department, KIMS hospital, Bangalore.
Table 3: Age distribution of patients
| Age in years | Non DM | DM | ||
| No | % | No | % | |
| 40-50 | 18 | 24.0 | 13 | 17.3 |
| 51-60 | 27 | 36.0 | 25 | 33.3 |
| 61-70 | 24 | 32.0 | 31 | 41.3 |
| 71-80 | 4 | 5.3 | 4 | 5.3 |
| 81-90 | 2 | 2.7 | 2 | 2.7 |
| Total | 75 | 100.0 | 75 | 100.0 |
| Mean ± SD | 58.69±9.46 | 60.72±9.92 | ||
Patients above 40 years were included in the study. Mean age of diabetic patients is 60.72 years (with standard deviation of 9.92 years) and that of non diabetic patients is 58.69 years (with standard deviation of 9.46 years).
Figure 21: Age distribution of patients
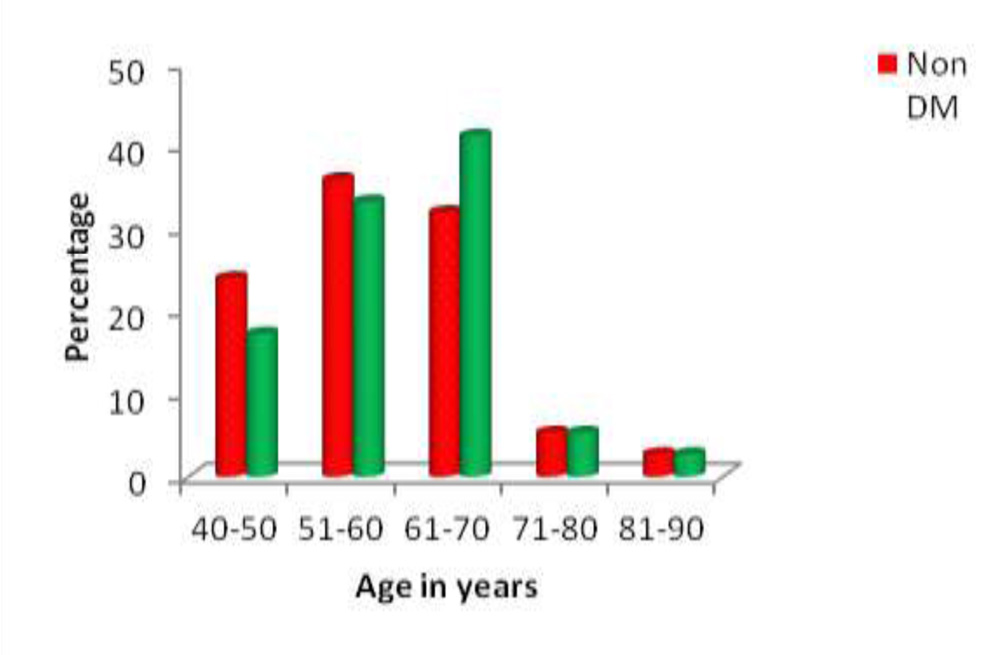
Maximum number of diabetic patients were in age group 61-70 years and non diabetic patients were in age group 51-60 years.
Table 4: Gender distribution of patients
| Gender | Non DM | DM | ||
| No | % | No | % | |
| Female | 38 | 50.7 | 41 | 54.7 |
| Male | 37 | 49.3 | 34 | 45.3 |
| Total | 75 | 100.0 | 75 | 100.0 |
Out of 75 diabetic patients, 41 were female and 34 were male. Out of 75 control group patients, 38 were female and 37 were male.
Figure 22: Gender distribution of patients 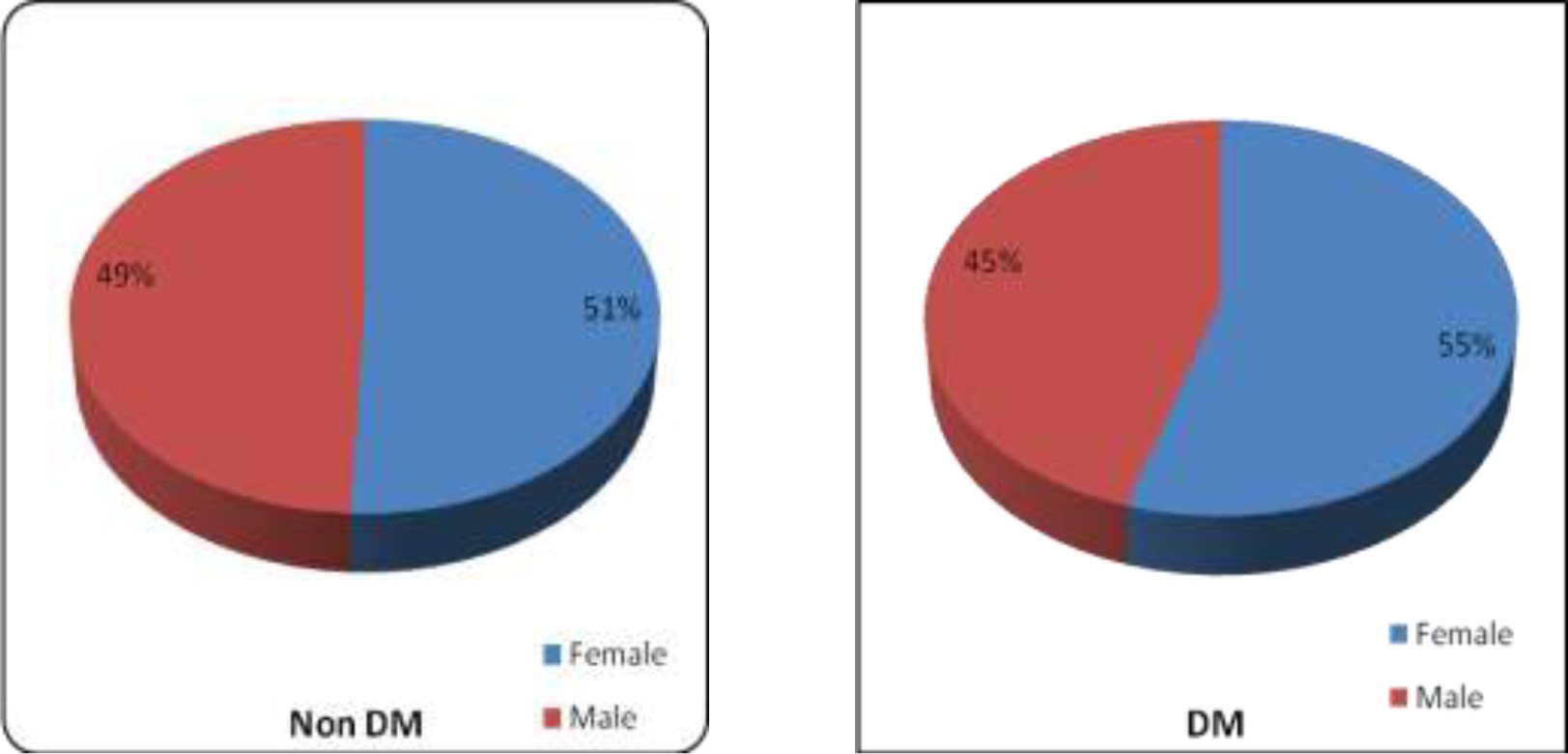
Table 5: Symptom Score of patients
| Symptom Score | Pre op | Post Op 1st Week | Post Op 3rd week | Post Op 6th week | % change |
| Non DM (n=75) | |||||
| · Absent | 68(90.7%) | 53(70.7%) | 58(77.3%) | 66(88%) | -2.7% |
| · Mild | 7(9.3%) | 15(20%) | 12(16%) | 6(8%) | -1.3% |
| · Moderate | 0(0%) | 7(9.3%) | 5(6.7%) | 3(4.0%) | 4.0% |
| · Severe | 0(0%) | 0(0%) | 0(0%) | 0(0%) | 0.0% |
| DM (n=75) | |||||
| · Absent | 52(69.3%) | 27(36%) | 32(42.7%) | 48(64%) | -5.3% |
| · Mild | 17(22.7%) | 20(26.7%) | 20(26.7%) | 17(22.7%) | 0% |
| · Moderate | 6(8%) | 21(28%) | 18(24%) | 7(9.3%) | 1.3% |
| · Severe | 0(0%) | 7(9.3%) | 5(6.6%) | 3(4%) | 4.0% |
Grades of dry eye symptoms in both groups pre and post operatively. Increased dry eye symptom seen in both groups post SICS with more pronounced result in DM.
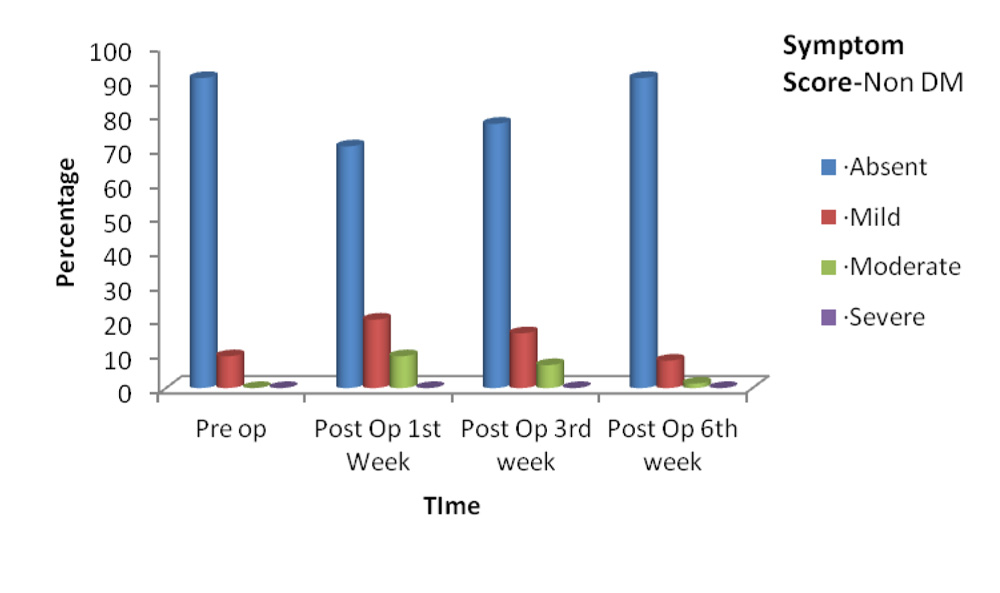
Figure 24: Symptom score grades among Non DM group (line diagram)
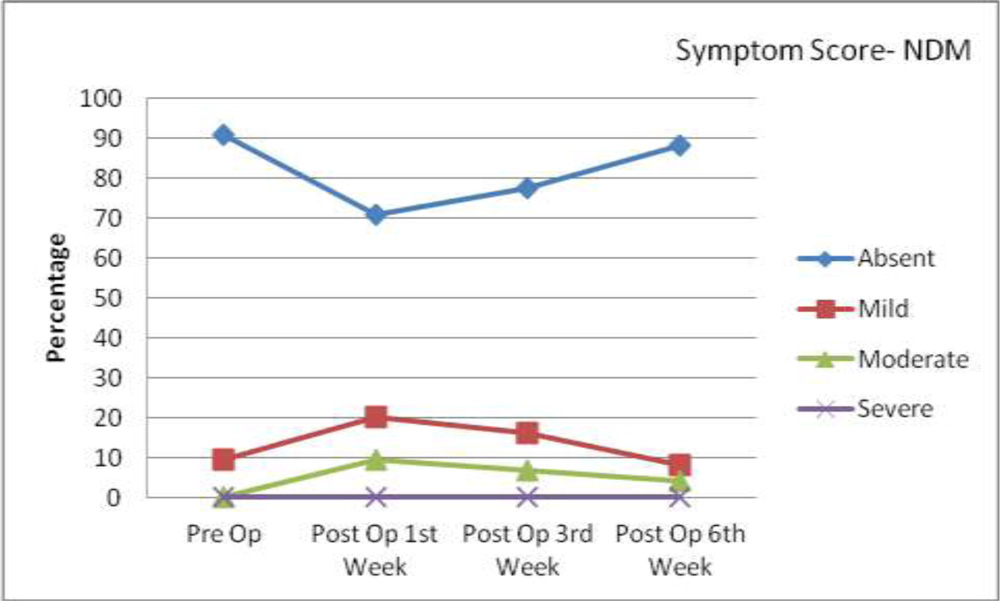
Above figures show percentage of patients in different symptom grades among Non DM group in form of bar chart and line diagram. These figures show that among Non DM dry eye symptom increased during 1st week and subsequently got reduced in 3rd and 6th week.
Figure 25: Symptom score grades among DM group (Bar Chart)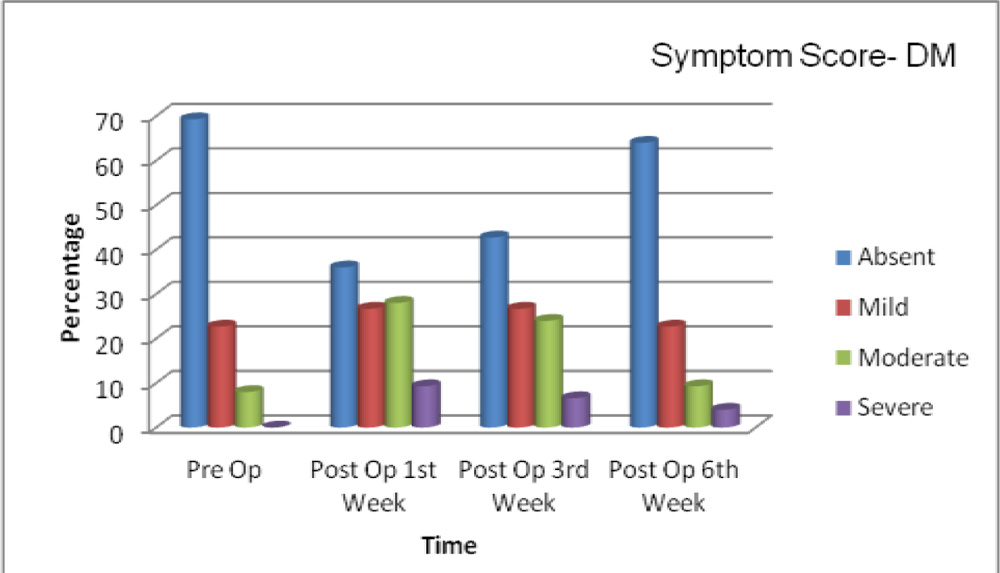
Figure 25: Symptom score grades among DM group (Bar Chart)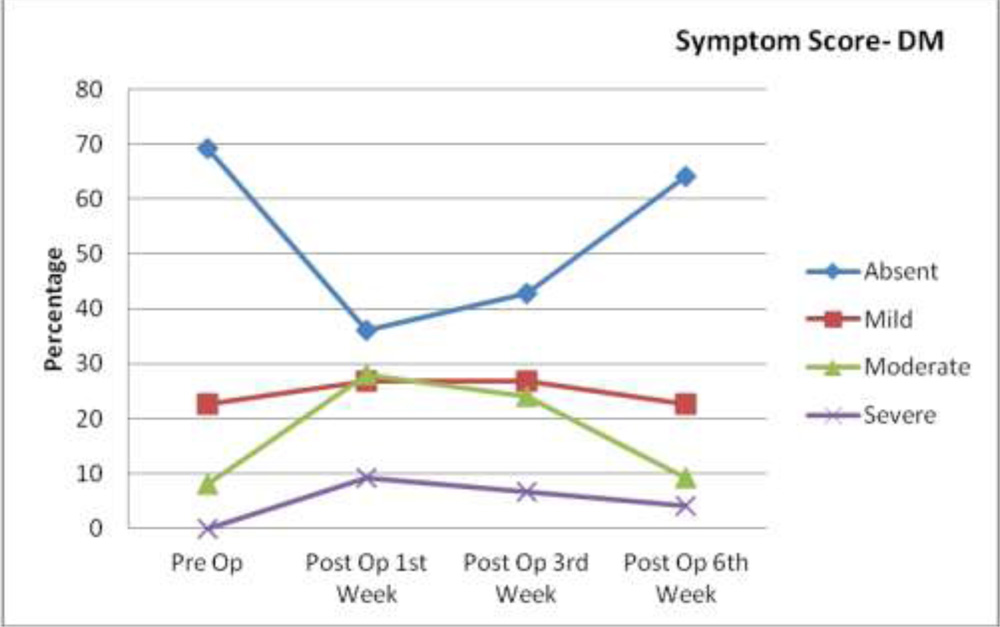
Above figures show percentage of patients in different symptom grades among DM group in form of bar chart and line diagram. Among DM group, dry eye symptom increased during 1st to 3rd week and shows a decreasing trend from 3rd to 6th week post operatively.
Table 6: Tear Break up Time (Sec.) of patients
| Tear Break Up Time | Non DM | DM | P value |
| Pre op | 16.91±5.97 | 13.12±5.58 | <0.001** |
| Post op 1st week | 8.60±4.20 | 5.04±2.47 | <0.001** |
| Post op 3rd weeks | 8.35±4.29 | 5.19±2.39 | <0.001** |
| Post op 6th week | 10.41±4.04 | 7.09±2.65 | <0.001** |
| Difference from Pre-op | |||
| · Post op 1st week | 8.307 | 8.080 | – |
| · Post op 3rd weeks | 8.560 | 7.933 | – |
| · Post op 6th week | 6.493 | 6.027 | – |
| P value from Pre-op | |||
| · Post op 1st week | <0.001** | <0.001** | – |
| · Post op 3rd weeks | <0.001** | <0.001** | – |
| · Post op 6th week | <0.001** | <0.001** | – |
TBUT among DM and Non DM group showing strong correlation with its pre OP value.
Figure 27 : Tear Break up Time (Sec.) of patients
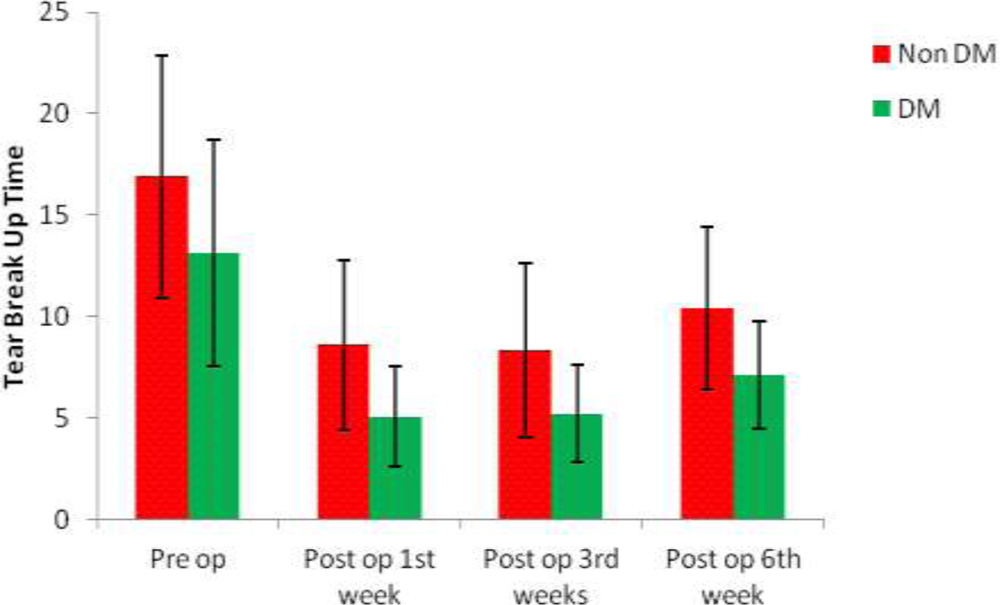
Table 7: Schirmer’s 1 Test values (mm) of patients
| Schirmer’s 1 Test | Non DM | DM |
| Pre op | 24.25±7.41 | 17.77±7.71 |
| Post op 1st week | 16.08±8.68 | 7.23±4.54 |
| Post op 3rd weeks | 14.48±6.89 | 7.51±3.35 |
| Post op 6th week | 15.88±6.14 | 10.76±3.87 |
| Difference from Pre-op | ||
| · Post op 1st week | 8.173 | 10.547 |
| · Post op 3rd weeks | 9.773 | 10.267 |
| · Post op 6th week | 8.373 | 7.013 |
| P value from Pre-op | ||
| · Post op 1st week | <0.04* | |
| · Post op 3rd weeks | <0.04* | |
| · Post op 6th week | <0.04* |
Sch 1 test value among DM group shows moderate correlation with its pre OP value.
Figure 28: Schirmer’s 1 Test values of patients
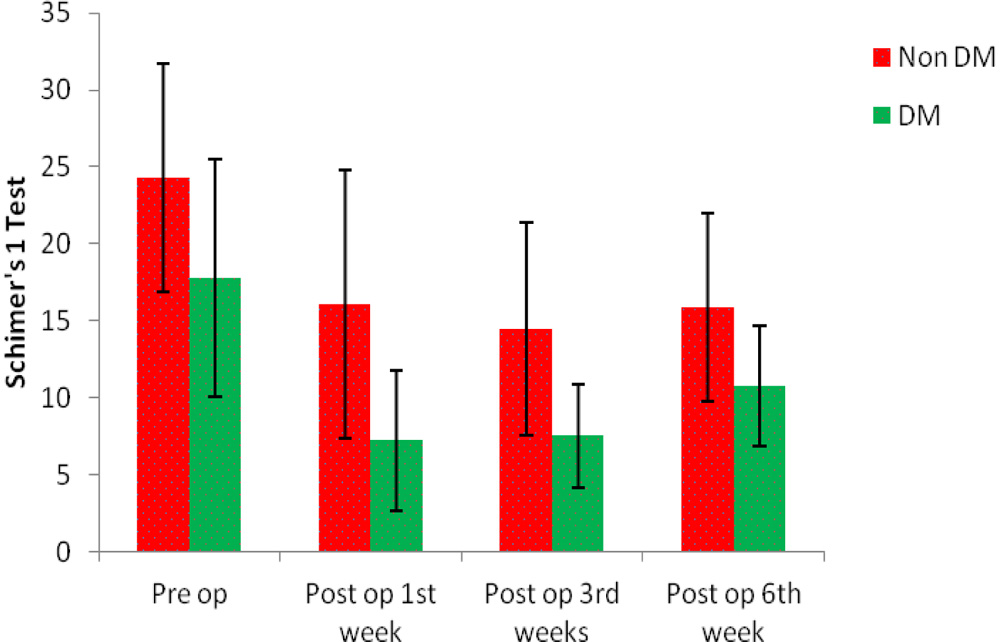
Table 8: Lissamine Green staining among patients
| Lissamine Green | Pre op | Post Op 1st Week | Post Op 3rd week | Post Op 6th week | % change |
| Non DM (n=75) | |||||
| · Negative | 74(98.7%) | 69(92%) | 70(93.33%) | 69(92%) | -6.7% |
| · Positive | 1(1.3%) | 6(8%) | 5(6.67%) | 6(8%) | 6.7% |
| DM (n=75) | |||||
| · Negative | 63(84%) | 53(70.67%) | 56(74.67%) | 54(72%) | -12% |
| · Positive | 12(16%) | 22(29.33%) | 19(25.33%) | 21(28%) | 12% |
| P value | 1.000 | 0.367 | 0.67 | 0.120 | – |
LG staining among DM and Non DM group showing no significant correlation.
Fig 29: Lissamine Green staining among Non DM patients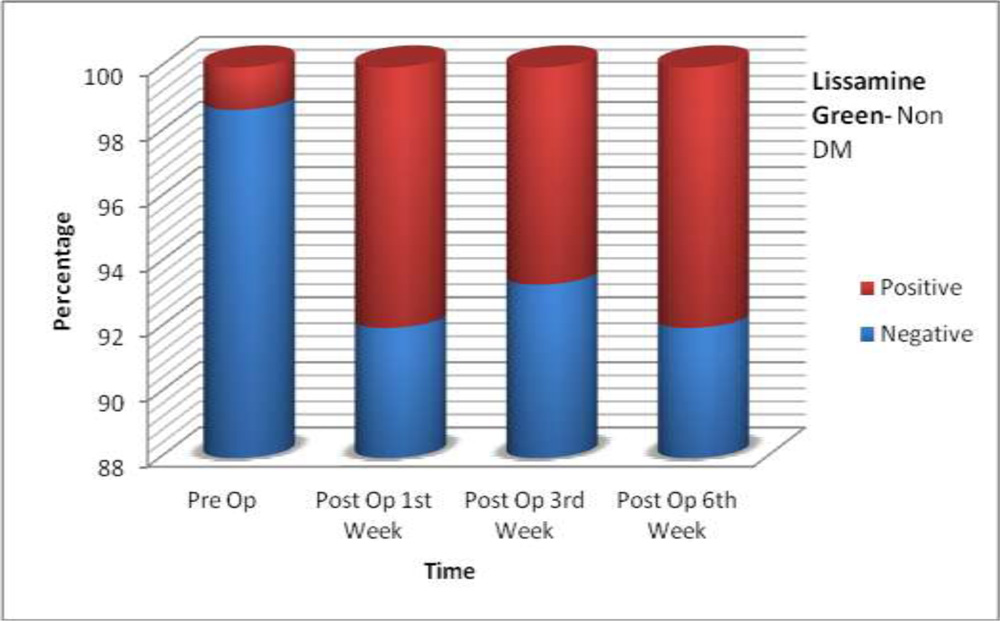
Fig 30: Lissamine Green staining among DM patients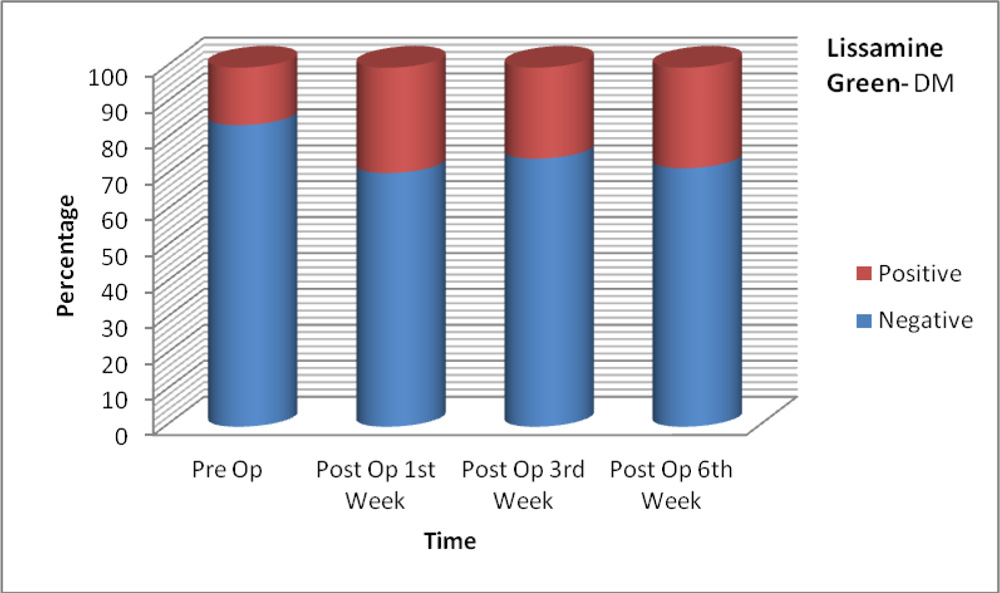
Table 9: Fluorescein Staining among patients
| Fluorescein Staining | Pre op | Post Op 1st Week | Post Op 3rd week | Post Op 6th week | % change |
| Non DM (n=75) | |||||
| · Negative | 75(100%) | 71(94.67%) | 70(93.33%) | 70(93.33%) | -6.67% |
| · Positive | 0 (0%) | 4(5.3%) | 5(6.67%) | 5(6.67%) | 6.67% |
| DM (n=75) | |||||
| · Negative | 69(92%) | 62(82.67%) | 64(85.33%) | 61(81.33%) | -9.3% |
| · Positive | 6(8%) | 13(17.83%) | 11(14.67%) | 14(18.67%) | 9.3% |
Positive corneal fluorescein staining observed pre operatively in DM group with marginal increase post operatively. No significant result in both groups.
Figure 31: Fluorescein Staining among Non DM group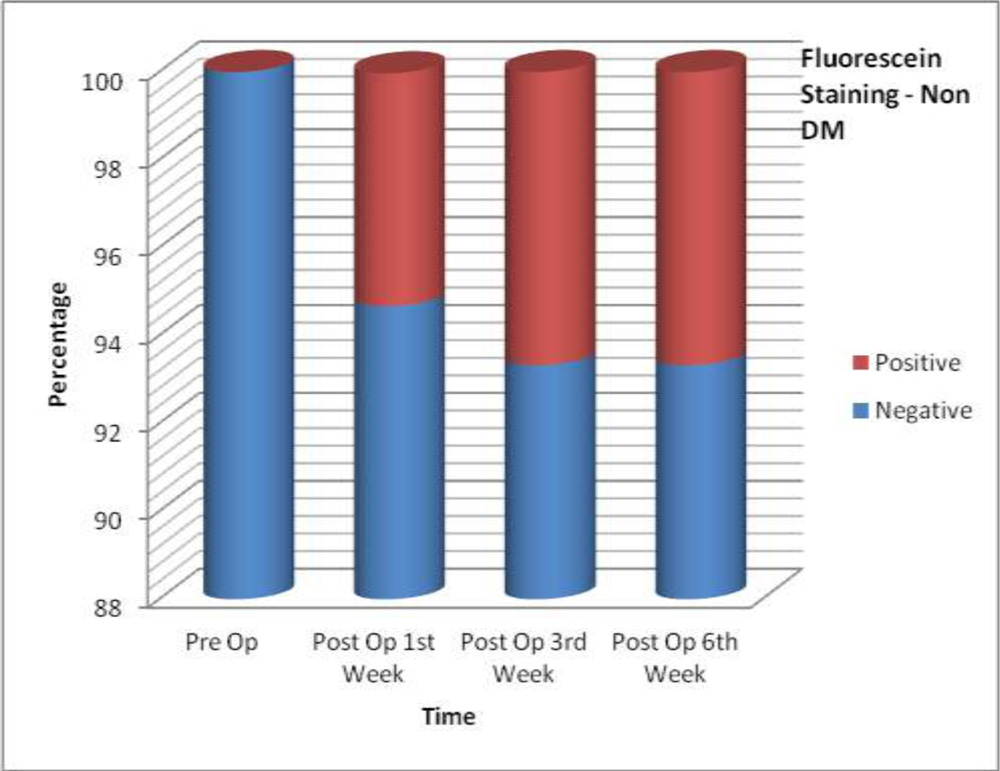
ong>Figure 32: Fluorescein Staining among DM group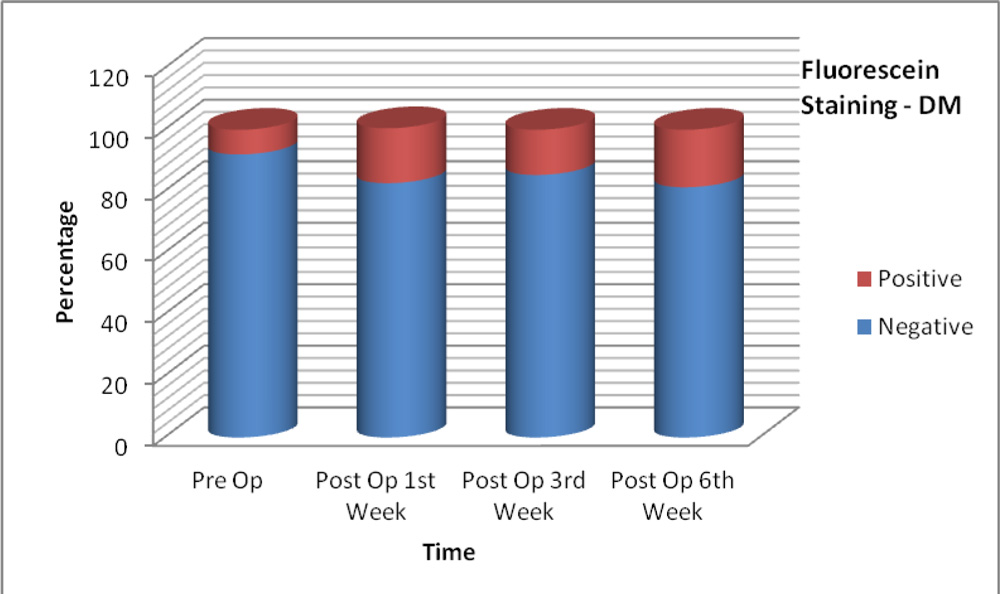
Table 10: Blink rate of patients
| Blink rate | Non DM | DM |
| Pre op | 15.48±2.64 | 12.87±3.32 |
| Post op 1st week | 15.60±3.00 | 13.09±3.68 |
| Post op 3rd weeks | 15.49±3.00 | 13.12±3.64 |
| Post op 6th week | 15.23±2.72 | 12.83±3.24 |
| Difference from Pre-op | ||
| · Post op 1st week | 0.120 | 0.227 |
| · Post op 3rd weeks | 0.013 | 0.253 |
| · Post op 6th week | 0.253 | 0.040 |
| P value from Pre-op | ||
| · Post op 1st week | 0.595 | 0.378 |
| · Post op 3rd weeks | 0.946 | 0.223 |
| · Post op 6th week | 0.140 | 0.735 |
P value was calculated which showed no significant correlation between pre OP and post OP values.
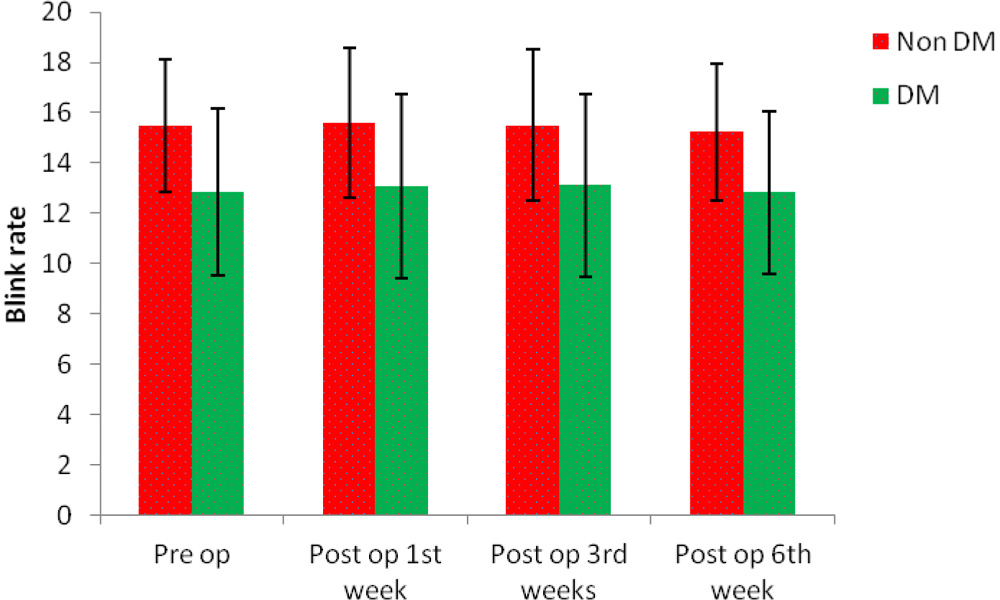
Table 11: Tear Meniscus Height of patients
| TMH | Pre op | Post Op 1st Week | Post Op 3rd week | Post Op 6th week |
| Non DM (n=75) | ||||
| Abnomal | 0(0%) | 7(9.33%) | 6(8%) | 2(2.67%) |
| Normal | 75(100%) | 68(90.67%) | 69(92%) | 73(97.33%) |
| DM (n=75) | ||||
| Abnomal | 3(4%) | 15(20%) | 16(21.33%) | 11(14.67%) |
| Normal | 72(96%) | 60(80%) | 59(78.67%) | 64(85.55%) |
TMH value among DM and Non DM group showing no significant finding.
Figure 34: Tear Meniscus Height among Non DM group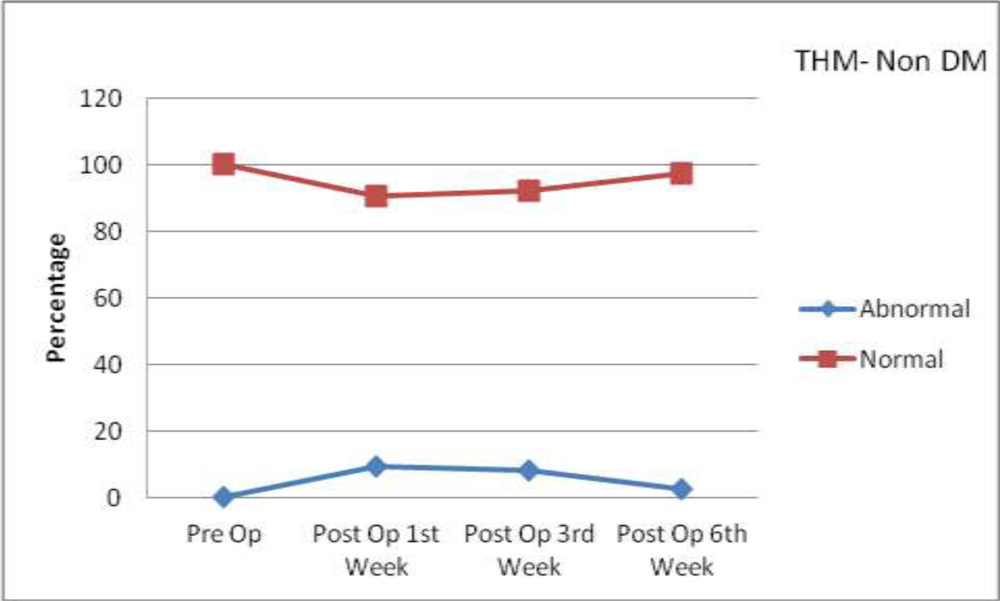
Figure 35: Tear Meniscus Height among DM group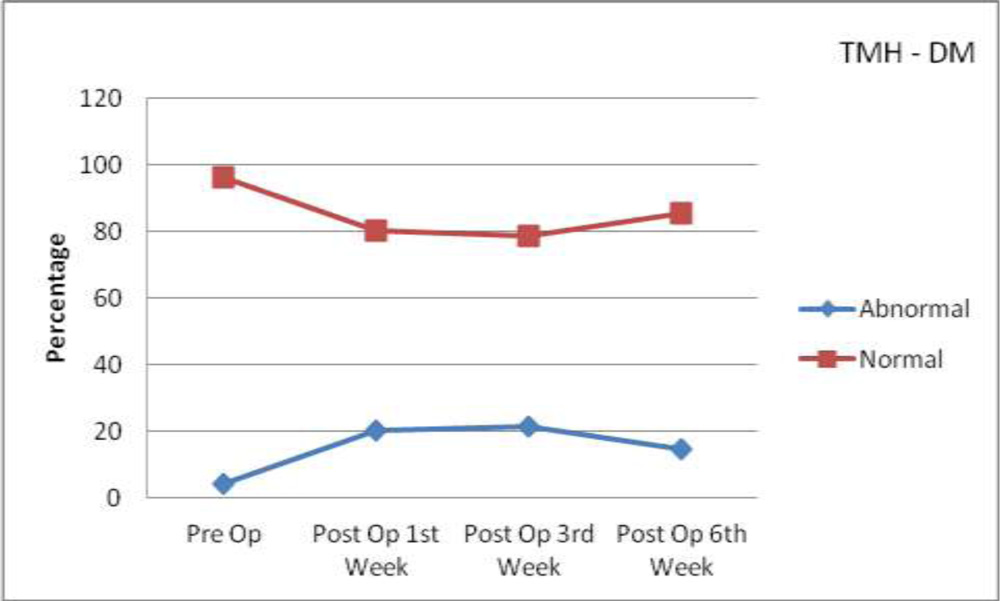
DISCUSSION
Dry eye disease is multifactorial disease of tear film and ocular surface that results in symptoms of discomfort, visual disturbance and tear instability with potential damage to the ocular surface which can aggravate following cataract surgery.
Cataract surgery is the most successful surgery in the field of ophthalmology and almost 20% of all cataract surgery are performed on diabetics.
In our study 150 eyes of 150 patients were enrolled. Patients with age above 40 years were selected for study with age from 40 to 85 years. Mean age of diabetic patients was 60.72 years (with standard deviation of 9.92 years) and that of non diabetic patients was 58.69 years (with standard deviation of 9.46 years).
In the study conducted by Ngamjit Kasetsuwan et al 80, mean age of patients who underwent cataract surgery was 67.22 years with std deviation of 8.26 with age between 42 to 84 yrs. In the study conducted by Kavitha C et al2, 68 patients in the age group of 40-80 years were selected. In study conducted by Ram et al81, all the patients were more than 40 years of age.
In our study, out of 150 patients, 79 were female. Majority of female population were housewives and farmers who had to work in dry, dusty environment and outdoor activities. Number of female patients was slightly higher than male patients.
In the study conducted by Ngamjit Kasetsuwan et al80 and Mohan S et al83, 66% and 58% of patients were female respectively. In the study conducted by Shankar S. et al82, out of 100 eyes of 100 patients 53 were female.
In our study, both DM and Non DM group showed increased dry eye symptoms during 1st Post operative week. Among Non DM patients, dry eye symptoms increased from 9.3% to 29.3% in 1st week post operatively. From 1st week post operatively (29.3%), Non DM group showed gradual decrease in dry eye symptoms in 3rd week (22.7%) and 6th week(12%).
In DM, 30.7% of patients showed dry eye symptoms pre operatively, which increased to 64% during 1st week post operatively. During 3rd week, dry eye symptoms showed marginal decrease from 1st week. It decreased to 57.33% from 64% during the period. During 6th week, dry eye symptoms came down to 36% which was slightly more than pre op values.
In the study conducted by Xi Liu et al7, both non-diabetic and diabetic patients had more severe dry eye symptoms on Days 1 to 7 postoperatively. Thereafter, the grades of dry eye symptoms returned to preoperative levels between Days 30 and 180 in the non-diabetic group, and however, remained elevated in diabetics even on day 180 postoperatively. Ocular symptom scores were significantly worse postoperatively than they were preoperatively.
Dandona et al.92, Peponis et al.93 and Yan et al.94, stated that diabetes mellitus is associated with increased oxidative stress and free radical production which can damage epithelial tissues, such as conjunctiva and lacrimal glands. Hence diabetic cataract patient will suffer more damage to the conjunctiva, lacrimal glands, goblet cells and peripheral nerve innervation to these structures, not only from diabetes mellitus per se, but also from the surgical procedure. Sitompul et al85, found that OSDI score decreased on day 14 in patients who had undergone SICS.
In our study, TBUT and correlation of post OP values with pre OP values among Non DM and DM was measured . TBUT decreased from 16.91 Sec (with standard deviation of 5.97 sec) to 8.60 sec (with standard deviation of 4.2 sec) among Non DM in 1st week. It again increased during 6th week post OP to 10.41 sec (with standard deviation of 4.04 sec). P value of post OP result with pre OP value was measured which showed strong correlation of TBUT in periods prior and post SICS.
Among DM, TBUT showed substantial decrease post OP with respect to pre OP value. TBUT decreased from 13.12 sec (with standard deviation of 5.58sec) to 5.04 sec (with standard deviation of 2.47 sec) during 1st week post OP. TBUT value showed slight improvement during 3rd week and significant improvement, 7.09 sec (with standard deviation of 2.65 sec) during 6th week. P value of post OP result with pre OP value was measured which showed strong correlation of TBUT in period prior and post SICS.
Ngamjit Kasetsuwan et al80,in their study, reported that the tear film instability in the operated eyes can result either from a surface irregularity at the site of the incision, which causes the tear film to break up faster than usual, or the mucin production from the conjunctiva may be decrease. Cho YK et al 86, concluded that vigorous irrigation of the tear film and manipulation of the ocular surface intraoperatively may reduce the goblet cell density and result in shortened TBUT postoperatively. Li XM et al10, proposed that Benzalkonium chloride, one of the most commonly used preservatives in topical eye drops, can induce tear instability and decrease the number of mucin expressing cells. Excessive instillation and incorrect use of preserved eye drops are important factors that contribute to the development of dry eye after phacoemulsification and corneal toxicity87.
Dogru 95 et al. reported previously that TBUT and Sch1 scores significantly decreased in non-insulin-dependent diabetes mellitus and suggested that diabetic neuropathy affected the innervation of the lacrimal gland, and that fluctuation in the glycemic control may affect the lacrimal gland secretory function. Furthermore, they also found a decrease in goblet cell numbers in diabetic patients, and hypothesized that this reduction in goblet cell numbers may account for the shortening of TBUT and instability of the tear film as a result of decreased mucin production.
In our study, Schimer’s 1 Test values were measured in both Non DM and DM groups pre and post SICS respectively. Among Non DM no significant result was observed pre and post SICS as values fall within normal range.
Among DM values decreased during post SICS period. During 1st week post SICS value decreased to 7.23 mm (with standard deviation of 4.54mm) from its pre OP value of 17.77 mm (with standard deviation of 7.71mm). The value slightly improved to 10.76mm (with standard deviation of 3.87mm) during 6th week post SICS. Among DM, there was moderate correlation of post SICS values with pre SICS values.
Goebbels et al90, reported that the SIT score significantly decreased while the TBUT value was unchanged in insulin-dependent diabetes, and suggested that the decreased SIT score indicated a decreased amount of reflex tearing due to a diminished corneal and conjunctival sensitivity in diabetics. It is suggested that diabetic cataract patient will suffer more damage to the conjunctiva, lacrimal glands, goblet cells and peripheral nerve innervation to these structures, not only from diabetes mellitus per se, but also from the surgical procedure. K E Han et al91, reported that Schirmer test did not show significant differences postoperatively.
In our study, lissamine green staining in Non DM group, 1.3% case showed positive result pre OP which increased to 8% . during 1st week. Lissamine green staining among DM, 16% cases showed positive result pre op which increased to 29.33% during 1st and 25.33% during 3rd week post operatively. During 6th week 28% cases showed positive staining with P value of 0.12 which shows no significant correlation of result with pre op value.
In our study, corneal fluorescein staining pre operatively was observed in DM group (8%) only. No positive staining was observed pre operatively in Non DM group. Among Non DM, fluorescein staining increased during 1st week and 3rd week post op which remained constant during 6th week. Among DM, fluorescein staining increased substantially during 1st week (17.83%) which reduced slightly during 3rd week (14.67%) and increased to 18.67% during 6th week.
In the study conducted by Kenneth A et al,84 mean corneal fluorescein staining was generally low across the study population (all subjects); no statistically significant differences were observed between patient groups. Mean conjunctival staining with lissamine green was more pronounced in both patient groups. Significantly higher mean conjunctival staining scores were observed in the diabetic patient group as compared with in the nondiabetic group (p value:0.034). The abnormal ocular surface staining in the current study showed typical interpalpebral staining pattern caused by dryness rather than inferior staining from drug toxicity or medicamentosa. The high incidence of abnormal Oxford Schema grading after phacoemulsification may be due to neurogenic inflammation.
In our study, blink rate values were recorded among Non DM and DM group during study period. P value was calculated which showed no significant correlation between pre OP and post OP values.
In our study, analysis of TMH among Non DM and DM groups was carried out. Among Non DM, no abnormal case was observed pre operatively. However during 1st week post OP 9.33% cases showed abnormal TMH value. Abnormal value got reduced to 8% and 2.67% during 3rd and 6th week respectively.
Among DM 4% cases showed abnormal TMH value during pre OP. This increased to 20% during 1st week and 21.33% during 3rd week. Percentage of abnormal cases reduced to 14.67% during 6th week. No correlation was found between pre operative values and post operative values during the study.
Hamid Gharaee et al.88, and Sitompul et al85, also reported that there was no statistically significant difference observed between pre and postoperative TMH results.
Mohana S et al 89, found that TMH values were found to be low preoperatively. The TMH values were lowest at 1 month, while it showed slight improvement at 3 months.
CONCLUSION
Among diabetic patients, the dry eye tests conducted on the eyes undergoing cataract surgery showed deterioration of TBUT and Sch 1 following surgery. Most severe value was recorded at 1st week post operatively. Thus it is seen that cataract surgery affected both tear quality and quantity among diabetic patients . Among non diabetic patients, the value of TBUT showed deterioration following surgery. Most severe value was recorded at 1st week post operatively which subsequently improved during 3rd and 6th week. Hence it is seen that cataract surgery affected tear quality to a certain extent even in non diabetic patients. Both Lissamine Green and fluorescein staining showed insignificant pattern at 6th week. In our study, both DM and Non DM group showed increased dry eye symptoms during 1st Post operative week. Among diabetic patients, increase was more during 1st week post operatively in comparison to non diabetic patients. The symptom score steadily decreased during 3rd and 6th week. Thus diabetic patients suffer more damage to tear film which is not only due to diabetes but also due to surgery. Our study indicates that SICS causes alteration in tear composition which results in unstable tear film.
The steroid drops and the other eye drops containing preservatives like benzalkonium chloride used in our setup could also be a contributing factor that leads to tear film instability. This contributes to the dry eye condition post operatively. Thus we conclude that SICS may cause or aggravate dry eye and affect the dry eye test values in the post operative period. Hence, before surgery, patients should be informed about the possible aggravation of dry eye symptoms and artificial tears should be prescribed for attenuating corneal damage and dry eye symptoms. If dry eye is detected preoperatively, artificial tears eyedrops can be prescribed.
SUMMARY
This This study “A Study To Assess The Effect Of Diabetes On Ocular Surface Disorder (OSD) After Small Incision Cataract Surgery And Its Management” was conducted in the Department of Ophthalmology, KIMS, Bangalore from December 2013 to May 2015 after obtaining clearance from the ethical committee.
This is a comparative hospital based study on 150 eyes of 150 patients undergoing small incision cataract surgery. Age distribution in the study was 40-85 years with female preponderance (55.3%). A detailed history was taken and a thorough ophthalmological examination was conducted.
The dry eye symptoms developed after cataract surgery had maximum severity at 1st Week in both DM (64%) and Non DM (29.3%). In diabetic patients, there was significant decrease in TBUT (5.04 Sec from 13.12 Sec) and Sch 1 (7.23mm from 17.77 mm) values at 1st week post operatively which improved during 3rd and 6th week. Both symptoms and signs improved over time in diabetic and non diabetic group. Post operative TBUT values showed strong correlation with its pre operative values in both diabetic and non diabetic group.
This study shows that SICS, due to various reasons already discussed, leads to dry eyes which has been proved by various tests showing altered parameter and further it was found that dry eye was more severe among DM patients compared to non DM.
BIBLIOGRAPHY
1.2007 Report of the International Dry Eye Work Shop (DEWS). (Special Issue) Ocul Surf 2007;5:75-174.
2.Kavitha C Venugopal, Pavana Acharya Krishnaraj, Chandan N. Evaluation of Dryness of Eyes after Manual Small Incision Cataract Surgery with Corneoscleral Tunnel Incision. Journal of Clinical and Diagnostic Research;2012 August;6(6):1029-1033.
3.Jack J Kanski, Brad Bowling.; Clinical Ophthalmology; 7th Elsevier; 2011.
4.Neena J, Rachel J, Praveen V, Murthy GV. Rapid Assessment of Avoidable Blindness in India, 2008; 3(8): e2867.
5.Onsiri Thanathanee, Terrence P. O’Brien. How Diabetes Impacts the Cornea and Ocular Surface; http://www.ophthalmologymanagement.com/articleviewer.aspx?articleID=104911; 11/1/2010.
6.Vasilis Achtsidis, Ioanna Eleftheriadou, Eleftheria Kozanidou, Konstantine Voumvourakis. Dry Eye Syndrome in Subjects With Diabetes and Association With Neuropathy. Diabetes Care; 2014;37:e210–e211 | DOI: 10.2337/dc14-0860
7.Xi Liu, Yangshun Gu, and Yesheng Xu. Changes of tear film and tear secretion after phacoemulsification in diabetic patients: J Zhejiang Univ Sci B.; 2008; 9(4); 324–328.
8.Nora Burda, Vilma Mema, Ejup Mahmudi, Brikena Selimi, Sulejman Zhugli, Basri Lenajni et al. Prevalence of dry eye syndrome at patients with diabetus melitus TIP 2; Journal of Acute Disease; 2013; Volume 2 (Issue 1); 48–51.
9.Sun XG, Zhonghua Yan Ke Za Zhi. Not to ignore the dry eye of cataract patients after surgery, 2008;44(4):291-2.
10.Li XM, Hu L, Hu J, Wang W. Investigation of dry eye disease and analysis of the pathogenic factors in patients after cataract surgery; Cornea;2007; 26; 16-20.
11.Oh T, Jung Y, Chang D, Kim J, Kim H. Changes in the tear film and ocular surface after cataract surgery; Jpn J Ophthalmol.2012 ;56(2); 113-8
12.Kyung-Chul Yoon, Seong-Kyu Im, Man-Seong Seo. Changes of tear film and ocular surface in diabetes mellitus; Korean J Ophthalmol 2004;18(2); 168-74.
13.Mackie IA, Seal DV. Diagnostic implications of tear protein profiles.Br J Ophthalmol 1984;68:321-4.
14.Herber S, Grus FH, Sabuncuo P, Augustin Two-dimensional analysis of tear protein patterns of diabetic patients. Electrophoresis 2001;22:1838-44.
15.Wolff E. The muco-cutaneous junction of the lid margin and the distribution of the tear fluid. Trans Ophthamol Soc 1946;66:291-308.
16.Tiffany J. Tear film stability and contact lens wear. J Br Contact Lens Assoc 1988;11:35-38.
17.Prydal JI, Campbell FW. Study of precorneal tear film thickness and structure by interferometry and confocal microscopy. Invest Ophthalmol Vis Sci 1992;33:1996-2005.
18.King-Smith PE, Fink BA, Fogt N, Nichols KK, Hill RM, Wilson GS. The thickness of the human precorneal tear film: evidence from reflection spectra. Invest Ophthalmol Vis Sci 2000;41:3348-59.
19.Anthony J Bron, Ramesh C Tripathi, Brenda J Tripathi. Wolff’s Anatomy of the Eye and Orbit. 8th Ed. Chapman and Hall; 1997.
20.Sullivan DA. Androgen deficiency and dry eye syndromes. Arch Soc Esp Oftalmol 2004;79:49-50.
21.Sullivan DA, Sullivan BD, Evans JE, Schirra F, Yamagami H, Liu M, Richards SM, Suzuki T, Schaumberg DA, Sullivan RM, Dana MR. Androgen deficiency, meibomian gland dysfunction, and evaporative dry eye. Ann N Y Acad Sci 2002; 966:211-22.
22.Daniel M Albert, Joan W Miller, Dimitri T Azar, Barbara A Blodi. Principles and Practice of Ophthalmology. 3rd ed. Elsevier; 2008.
23.Yokoi N, Takehisa Y, Kinoshita S. Correlation of tear lipid layer interference patterns with the diagnosis and severity of dry eye. Am J Ophthalmol 1996;122:818-24.
24Hodges RR, Dartt DA. Keratoconjunctivitis sicca: Physiology and Biochemistry of the Tear Film. In: J.H. Kracmer, M.J. Mannis, and E.J. Holland, eds. Cornea. Philadelphia: Lippincott Williams and Wilkins; 2005:577-602.
25.Yamada M, Mochizuki H, Kawai M, Yoshino M, Mashima Y. Fluorophotometric measurement of pH of human tears in vivo. Curr Eye Res 1997;16:482-6.
26.Seal DV, McGill JI, Mackie IA, Liakos GM, Jacobs P, Goulding NJ. Bacteriology and tear protein profiles of the dry eye. Br J Ophthalmol 1986;70:122-5.
27.Avisar R, Menache R, Shaked P, Rubinstein J, Machtey I, Savir H. Lysozyme content of tears in patients with Sjogren’s syndrome and rheumatoid arthritis. Am J Ophthalmol 1979;87:148-51.
28.Ohashi Y, Ishida R, Kojima T, Goto E, Matsumoto Y, Watanabe K, Ishida N, Nakata K, Takeuchi T, Tsubota K. Abnormal protein profiles in tears with dry eye syndrome. Am J Ophthalmol 2003;136:291-9.
29.Gipson IK, Argueso P. Role of mucins in the function of the corneal and conjunctival epithelia. Int Rev Cytol 2003;231:1-49.
30.Gipson IK. Distribution of mucins at the ocular surface. Exp Eye Res 2004;78:379-88.
31.Gum JR, Jr. Human mucin glycoproteins: varied structures predict diverse properties and specific functions. Biochem Soc Trans 1995;23:795-9.
32.Jay H Krachmer, Mark J Mannis, Edward J Holland. Cornea. 3rd ed. Elsevir, 2011.
33.Lemp MA. Report of the National Eye Institute/Industry Workshop on Clinical Trials in Dry Eye. CLAO J 1995;21:221-32.
34.Behrens A, Doyle JJ, Stern L, et al. Dysfunctional tear syndrome: A Delphi approach to treatment recommendations. Cornea 2006;25:900-7.
35.Preferred Practice Pattern Series #1 Dry Eye Disease; All India Ophthalmic Society; 2013 July; 2-7.
36.Schaumberg DA, Sullivan DA, Buring JE, Dana MR. Prevalence of dry eye syndrome among US women. Am J Ophthalmol 2003; 136: 318-26.
37.Bukhari A, Ajlan R, Alsaggaf H. Prevalence of dry eye in the normal population in Jeddah, Saudi Arabia. Orbit 2009; 28: 392-7.
38.Basak SK, Pal PP, Basak S, Bandyopadhyay A, Choudhury S, Sar S. Prevalence of Dry Eye Diseases in hospital-based population in West Bengal, Eastern India. J Indian Med Assoc. 2012; 110: 789-94.
39.Liotet S, Van Bijsterveld OP, Kogbe O, Laroche L. A new hypothesis on tear film stability. Ophthalmologica 1987;195:119-24.
40.Sharma A, Ruckenstein E. Mechanism of tear film rupture and its implications for contact lens tolerance. Am J Optom Physiol Opt 1985;62:246-53.
41.Battat L, Macri A, Dursun D, Pflugfelder SC. Effects of laser in situ keratomileusis on tear production, clearance, and the ocular surface. Ophthalmology 2001;108:1230-5.
42.Albietz JM, Lenton LM, McLennan SG. Effect of laser in situ keratomileusis for hyperopia on tear film and ocular surface. J Refract Surg 2002;18:113-23.
43.Skyberg K, Skulberg KR, Eduard W, Skaret E, Levy F, Kjuus H. Symptoms prevalence among office employees and associations to building characteristics. Indoor Air 2003;13:246-52.
44.McCulley JP, Aronowicz JD, Uchiyama E, Shine WE, Butovich Correlations in a change in aqueous tear evaporation with a change in relative humidity and the impact. Am J Ophthalmol 2006;141:758-60.
45.Myron Yanoff, Jay S Duker. Ophthalmology. 3rd ed. Elsevier; 2009.
46.James DG, Anderson R, Langley D, Ainslie D. Ocular Sarcoidosis. Br J Ophthalmol 1964; 48:461-70.
47.Obata H, Yamamoto S, Horiuchi H, Machinami R. Histopathologic study of human lacrimal gland. Statistical analysis with special reference to aging. Ophthalmology. 1995;102:678–686.
48.Kaiserman I, Kaiserman N, Nakar S, Vinker S. Dry eye in diabetic patients. Am J Ophthalmol. 2005;139:498–503.
49.Cavanagh HD, Colley AM. The molecular basis of neurotrophic keratitis. Acta Ophthalmol Suppl. 1989;192:115–134.
50.Moss SE, Klein R, Klein BE. Incidence of dry eye in an older population. Arch Ophthalmol. 2004;122: 369–373.
51.Foulks G, Bron AJ. A clinical description of meibomian gland dysfunction. Ocul Surf. 2003:107–126.
52.American Academy of Ophthalmology Panel. Preferred Practice Pattern Guidelines. Dry Eye Syndrome. San Francisco, CA: American Academy of Ophthalmology; 2008; 7-8.
53.Yokoi N, Bron AJ, Tiffany JM, Maruyama K, Komuro A, Kinoshita S. Relationship between tear volume and tear meniscus curvature. Arch Ophthalmol. 2004;122:1265–1269.
54.Mainstone JC, Bruce AS, Golding TR. Tear meniscus measurement in the diagnosis of dry eye. Curr Eye Res. 1996;15:653–661.
55.Norn MS. Desiccation of the precorneal tear film. I. Corneal wetting time. Acta Ophthalmol (Copenh). 1969;47:865–880.
56.Lemp MA, Hamill JR. Factors affecting tear film breakup in normal eyes. Arch Ophthalmol. 1973;89:103–105.
57.Van Bijisterveld OP. Diagnostic tests in sicca syndrome. Arch Ophthalmol. 1969;82:10–14.
58.Jones LT. The lacrimal secretory system and its treatment. Am J Ophthalmol. 1966;62:47–60.
59.Hamano H, Hori M, Hamano T, et al. A new method for measuring tears. CLAO J. 1983;9:281–289.
60.Foulks GN. Challenges and pitfalls in clinical trials of treatments for dry eye. Ocul Surf. 2003;1:20–30.
61.Bron AJ, Evans VE, Smith JA. Grading of corneal and conjunctival staining in the context of other dry eye tests. Cornea 2003;22:640-50.
62.Xu KP, Yagi Y, Toda I, et al. Tear function index: a new measure of dry eye. Arch Ophthalmol. 1995;113:84–88.
63.Tomlinson A, McCann L, Pearce I. Comparison of OcuSense and Clifton nanolitre osmometers. ARVO Abstract, 2009
64.Goto E, Ishida R, Kaido M, et al. Optical aberrations and visual disturbance associated with dry eye. Ocul Surf. 2006;4(4):207–213.
65.Bron AJ, Benjamin L, Snibson GR. Meibomian gland disease. Classification and grading of lid changes. Eye. 1991;5:395–411.
66.Yamada N, Yanai R, Inui M, Nishida T. Sensitizing effect of substance P on corneal epithelial migration induced by IGF-1, fibronectin, or interleukin-6. Invest Ophthalmol Vis Sci. 2005;46:833– 839.
67.Asbell PA. Increasing importance of dry eye syndrome and the ideal artificial tear: consensus views from a roundtable discussion. Curr Med Res Opin. 2006;22:2149–2157.
68.Argueso P, Tisdale A, Spurr-Michaud S, et al. Mucin characteristics of human corneal-limbal epithelial cells that exclude the rose bengal anionic dye. Invest Ophthalmol V is Sci. 2006;47:113–119.
69.Murakami T, Fujihara T, Horibe Y, Nakamura M. Diquafosol elicits increases in net Cl- transport through P2Y2 receptor stimulation in rabbit conjunctiva. Ophthalmic Res. 2004;36:89–93.
70Kojima T, Higuchi A, Goto E, Matsumoto Y, Dogru M, Tsubota K. Autologous serum eye drops for the treatment of dry eye diseases. 2008;27(Suppl 1):S25–S30.
71.López-García JS, García-Lozano I, Rivas L, Martínez-Garchitorena J. Use of autologous serum in ophthalmic practice. Arch Soc Esp Oftalmol 2007;82(1):9-20
72.Alio JL. Treatment of Ocular Surface Syndrome After LASIK With Autologous Platelet-rich Plasma. Journal of Refractive Surgery 2007;23.
73.Sahlin S, Linderoth R. Eyelid botulinum toxin injections for the dry eye. Dev Ophthalmol 2008; 41: 187-92.
74.Ashok Garg. Ocular Therapeutics. 3rd ed. Jaypee Publishers; 2013.
75.Penny A Asbell, Michael A Lemp. Dry Eye Disease. Thieme Medical Publisher Inc.;2006.
76.Bernard Rosner, Fundamentals of Biostatistics, 5th Edition, Duxbury, 2000.
77.Robert H Riffenburg , Statistics in Medicine , second edition, Academic press, 2005.
78.Sunder Rao P S S , Richard J : An Introduction to Biostatistics, A manual for students in health sciences , New Delhi: Prentice hall of India. 4th edition,
79.Suresh K.P. and Chandrasekhar S. Sample Size estimation and Power analysis for Clinical research studies. Journal Human Reproduction Science, 2012;5(1), 7-13.
80.Ngamjit Kasetsuwan, Vannarut Satitpitakul, Theerapa Changul, Supharat Jariyakosol. Incidence and Pattern of Dry Eye after Cataract Surgery. PLOSONE; November 2013; 8( 11) :1-6.
81.Ram J, Gupta A, Brar GS, Kaushik S, Gupta A. Outcomes of phacoe-mulsification in patients with dry eye. J Cataract Refract Surg. 2002 March; 28: 1386-1389.
82.Shankar S. Ganvit, H D Ahir, Jayesh Sadhu, Pandey NN. Study of the dry eye changes after cataract surgery. Int J Res Med. 2014; 3(2):1421-45.
83.Mohana Sinha, Abhik Sinha, Dibakar Haldar, Sanchari Roy, Bithi Chowdhury , Saibendu Kumar Lahiri. Demography and Characterisation of Visual Acuity in Preoperative and Postoperative Period of Cataract Surgery. IOSR Journal of Dental and Medical Sciences; May. 2015;14(5), 24-28.
84.Kenneth A. Beckman. Characterization of Dry Eye Disease in Diabetic Patients Versus Non diabetic Patients. Cornea 2014; 33: 851–854
85.Sitompul R, Sancoyo GS, Hutauruk JA, Gondhowiardjo TD. Sensitivity Change in Cornea and Tear layer due to Incision Difference on Cataract Surgery with Either Manual Small-Incision Cataract Surgery or Phacoemulsification. Cornea. 2008 Sep; 27:13-18
86.Cho YK, Kim MS. Dry eye after cataract surgery and associated intraoperative risk factors. Korean Journal of Ophthalmology; 2009; 23: 65-73.
87.Wilson WS, Duncan AJ, Jay JL. Effect of benzalkonium chloride on the stability of the precorneal tear film in rabbit and man. Br J Ophthalmol. 1975 Nov; 59(11): 667–669.
88.Hamid Gharaee, Mir Naghi Mousavi, R Daneshvar, M Hosseini, S Sazande. Effect of Clear Corneal Incision Location on Tear Film following Phacoemulsification Surgery. Irani Journal of Ophthalmology, 2009; 21(3): 29-34.
89.Mohana Sinha, Abhik Sinha, Bithi Chowdhury. Comparative Evaluation of Dry Eye Following Cataract Surgery: A Study from North India. IOSR Journal of Dental and Medical Sciences; Jun. 2014;Volume 13; Issue 6: 13-18.
90.Goebbels, M. Tear secretion and tear film function in insulin dependent diabetics. Br. J. Ophthalmol., 2008; 4(1): 19-21.
91.K E Han, S C Yoon, J M Ahn, S M Nam. Evaluation of Dry Eye and Meibomian Gland Dysfunction After Cataract Surgery. American Journal of Ophthalmology; June 2014; 157: 1144-50.
92.Dandona P., Thusu K., Cook S., Snyder B, Makowski, J., Armstrong, D., Nicotera, T. Oxidative damage to DNA in diabetes mellitus. Lancet; 1996; 347(8999): 445-447.
93.Peponis V., Papathanasiou M., Kapranou A., Magkou G., Tyligada A., Melidonis A., Drosos T., Sitaras N.M.,. Protective role of oral antioxidant supplementation in ocular surface of diabetic patients. Br. J. Ophthalmol. 2002; 86(12): 1369-1373.
94.Yan D., Schmidt A.M,, Anderson G.M., Zhang J., Brett J., Zou Y.S., Pinsky D., Stern D.. Enhanced cellular oxidant stress by the interaction of advanced glycation and products with their receptors/binding proteins. J. Biol. Chem. 1994, 269(13):9889-9897
95.Murat Dogru, Chikako Katakami, Masanori Inoue. Tear Function and Ocular Surface Changes in Noninsulin-dependent Diabetes Mellitus. Ophthalmology March 2001; 108(3):586-92.