 FP687 : Do All Dry Eye Complain Patients Have Really Dry Eyes?
FP687 : Do All Dry Eye Complain Patients Have Really Dry Eyes?![]()
AIOS – Comprehensive Ophthalmology Award
Dr. Revathy
Subramany, S14321, Dr. Hassan H Al Arrayed
Abstract
Aim:
To study the Tear analysis in patients complaining of dry eye.
Method:
A prospective study performed on 460 consecutive patients who had complaints of dry eye. All were subjected to tear analysis by Schirmers test, tear lab (Osmolarity) and keratography (aqueous layer, mucin layer, lipid layer), and Tear Break Up time (TBU).
Results :
19.51% patients were affected by all components and are considered as dry eyes; 17.07% didn’t show dry eye ; 24.39% had aqueous; 9.73% lipid and 7.3% mucin deficiency ; 9.76% had mucin with aqueous; 12.24% had lipid with aqueous & 9.73% had lipid with mucin deficiency. Osmolarity was high in 50% aqueous deficient patients, in 100% lipid deficient & severe dry eye patients.
Conclusion:
83% patients had dry eye. Aqueous component deficiency was more common and is observed in post LASIK and contact lens wear patients. Menopause and Meibomian gland diseases are related to lipid deficiency.
Ahealthy tear film is required for the normal function and health of the eye.Adequate production of tears, retention onthe ocular surface, and balanced evaporation are essential for the normal tear film dynamics. Dry eye syndrome (DES) is characterized by instability of the tear film that can be due to insufficient amount of tear components production or due to poor quality of tear film, which results in increased evaporation of the tears. DES is also called keratoconjunctivitissicca (KCS), keratitis sicca,sicca syndrome, xerophthalmia, dry eye disease (DED),ocular surface disease (OSD), or dysfunctional tear syndrome (DTS), or simply dry eyes [1].Dry eye can mainly bedivided into two groups, namely,(1) aqueous production deficient dry eye disease;(2) evaporative dry eye disease.
Insufficient tears cause damage to the interpalpebral ocularsurface and are associated with symptoms of discomfort.Both aqueous-deficient and evaporative dry eye can lead to increased evaporation and decreased tear film stability. Distinguishing between these two groups and determining if they exist individually or as a combination is crucial for DED diagnosis and treatment.The International Dry EyeWorkshop (2007) defined dry eyeas a multifactorial disease of the tears and ocular surfacethat results in symptoms of discomfort, visual disturbance,and tear film instability with potential damage to the ocular surface.It is accompanied by increased osmolarity of thetear film and inflammation of the ocular surface [1, 2].DES is associated with disturbances in quality of vision as tear films plays a cardinal role in maintain the optical property of cornea . As a result the activities such as reading, driving, and computer relatedwork, which require visual attention is affected. Patients experience dryeyes symptoms constantly and severely, affecting their qualityof life 3-7.
Components of tears affecting performance
The tear film is a very complex structure made up of numerous different components, such as lipids, proteins, salts, minerals,mucin and water, whose interactions are essential to its stability.Table 1
The aqueous layer or watery part of the tear film is produced by the lacrimal glands. This is the thick middle layer of the tear film. The mucin layer underneath helps it adhere to the epithelium and the lipid layer on top protects it from rapid evaporation.Aqueous teardeficient dry eye implies that dry eye is due to a failure of lacrimal tear secretion. In any form of dry eye due to lacrimal acinar destruction or dysfunction, dryness results from reduced lacrimal tear secretion and volume.8,9This causes tear hyperosmolarity.Although the water evaporates from the ocular surface at normal rates, it is from a reduced aqueous tear pool. Tear film hyperosmolarityaffects the ocular surface epithelial cells and stimulates a cascade of inflammatory events involving MAP kinases and NFkB signaling pathways10,11and the generation of inflammatory cytokines(interleukin (IL)-1?; -1?; tumor necrosis factor (TNF)-?)and matrix metalloproteinases (MMP-9 )12.
A lipid layer disturbance leads to an excessive evaporation rate and damage to the eye surface due to the resulting increased osmolarity13,14.An intact lipid layer can reduce the evaporation rate of tear fluid by 90-95% 15Further, it ensures a smooth surface of the tear film and is therefore critical for the quality of vision. In addition, the spreading of the lipid layer reduces free energy at the tear film surface and reduces surface tension by 25%, which is crucial for the structure of the entire tear film16.lipids come both from the Meibomian glands and lipocalin-associated, apparently delivered with the protein from the lacrimal gland21.
One of the major components of the tear film is Mucins which is a high-molecular-weight glycoprotein, found on the ocular surface are primarily produced by goblet cells, apical cells of the conjunctiva and cornea and the lacrimal glandGoblet cells primarily produce the gel-forming secretory mucin MUC5AC, the only gel-forming mucin of the ocular surface to be identified. Secretion typically occurs in response to a stimulus, such as a foreign body on the ocular surface. Thus, parasympathetic nerves act on these cells to stimulate mucus secretion. To prevent overstimulation and depletion of mucin from these cells, the number of goblet cells that respond to a neural stimulus must be regulated.17.Meanwhile, the apical cells of the conjunctiva and cornea produce the membrane-bound mucins MUC1, MUC2 and MUC4. These mucins primarily form the glycocalyx that protects the ocular surface. Finally, the lacrimal gland produces MUC7, a soluble secreted mucin that forms a part of the mucus layer18.This mucin is also found in the aqueous layer.
Decreased mucin levels have been found to be associated with dry eye. In dry-eye patients, the decreased levels of mucin are correlated with a decreased density of goblet cells. As the dry eye progresses, squamous metaplasia of the conjunctival cells occurs. The epithelial cells flatten and increase in area and the goblet cell density decreases.19It’s been found that vitamin A deficiencies, topical medications, excessive dosing with drops containing preservatives and cicatrizing conjunctival disorders can all damage goblet cells and the ocular surface. It’s important to note that vitamin A is essential for maintaining goblet cells and mucins on the ocular surface20.
Minerals
The electrolytes are principally Na, K, Cl_, and HCO_, with lower levels of Mg2 and Ca2; as secreted, tears are isotonic with serum although the proportions of ions are somewhat different, especially K. Many of the small molecules, such as glucose, lactate, urea, etc., also occur in serum but at different levels. More proteins can be detected (some estimates suggest as many as 80–100) but only four are present in large amounts, secreted from the lacrimal gland, its ductal epithelium and associated plasma cells (lysozyme, lactoferrin, lipocalin, and sIgA);
A growing number of people are landing in their doctor’s office complaining of gritty, irritated and dry eyes . Do all they have real dry eyes? This study is to assess the prevalence of anomalies in the components of tear film in patients complaining of dry eye.
Table 1 composition of human tears
| Water |
| Electrolytes |
| Proteins (lysozyme, lactoferrin, lipocalin, secretory IgA) |
| – albumin, IgG (leakage from conjunctiva) |
| Lipids (meibomian glands, lipocalin-associated) |
| Mucins (epithelial membrane-anchored type, soluble goblet-celltype) |
| Defensins, collectins, other small molecules |
MATERIALS AND METHODS
Patient selection
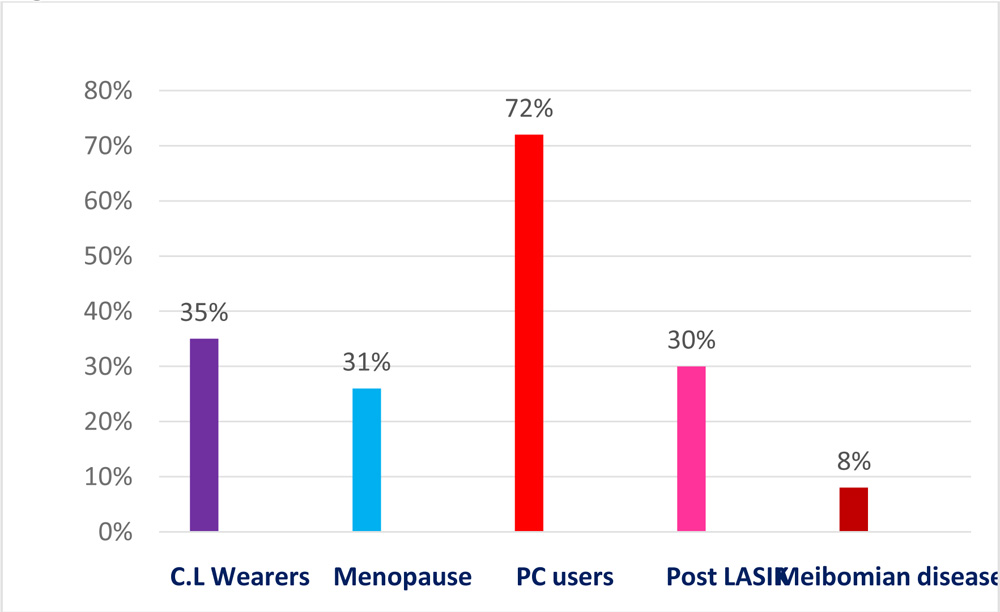
A prospective study performed on 460 patients visited the clinic with the complaints of dry eye. Depends on the structured questionnaire related to the predisposing factors, they are classified into 5 groups (Fig.1). Group 1 Post LASIK patients 30%; Group2 Contact lens wearers 35%; 72% were in Group3with prolonged hours of PC and smart phone users; Meibomian gland dysfunction patients were 8% and 31% patients reached menopause .All were subjected to tear analysis by schirmers test, tear lab and keratograph. Precorneal tear film (aqueous layer, mucin layer, lipid layer), Osmolarity and Tear Break Up time (TBU).
Fig:1 PATIENT’S DISTRIBUTION
Dry eye study
Dry eye work up included history collection, signs and symptoms and quantitative and qualitative analysis of tears..
Tear analysis
Tear analysis assessment includes aqueous layer, mucin layer, lipid layer and tear break up time(TBU)was assessed by Keratograph 5M (Occulus).
Schirmer Test.
Schirmer test quantitatively measures thetear production by the lacrimal gland during fixed timeperiod22,23. The basic test is performed without instilling topicalanaestheticby placing a thin strip of filter paper inthe inferior cul-de-sac .The patient’s eyes are closedfor 3 minutes and the amount of tears that wets the papers measured in terms of length of wet strip.Wetting of <15mm after 3minutes is considered abnormal. Value ofless than 6mm of strip wetting in 3 minutes is accepted asdiagnostic marker for aqueous tear deficiency.
Tear osmolarity
Tear osmolarity provides a single measurement that may reflect the balanceof input and output from tear dynamics. Osmolarity is the end product ofvariations in tear dynamics. Normal homeostasis requires regulated tear flow,the primary driver of which is osmolarity.24.Tear hyperosmolarity is the primary cause of discomfort, ocular surface damage, and inflammation in dry eye.25-27Tearosmolarity test was performed byTearLabosmometer (TearLab Corporation)theTearLabosmometer uses a so-called “lab on a chip” at the tip of a handheld sampler. The “lab on a chip” is a single-use microchip embedded with gold electrodes that measure the electrical impedance of the tear fluid sample in a tiny channel in the chip.
The electrical impedance osmometer takes an almost microscopic sample, just 50 nanoliters.To perform the test, the clinician uses the handheld sampler to collect a very small sample of tear fluid—just 50nL. The clinician placed the tip of the handheld device adjacent to the inferior lateral meniscus of the tear film, and then the correct amount of fluid is absorbed onto the microchip by passive capillary action.The handheld sampler is then docked into the stationary reader. Inside the handheld device, the gold-plated microchip measures the electrical impedance, and then the reader calculates and displays the osmolarity measurement in just a few seconds.Osmolarity of normal eye is 309–316mOsm/L and the value increases with severity of dry eye disease. It gives qualitative information of tear production. It is a very sensitive test but lacks specificityconcluded from a multicenter28.
- 316mOsmol/L and higher indicates dry eye (hyperosmolarity
- 290mOsmol/L to 316mOsmol/L suggests borderline or intermittent dry eye.
- 290mOsmol/L and below is healthy and normal29.
Tear Film Breakup Time (TBUT).
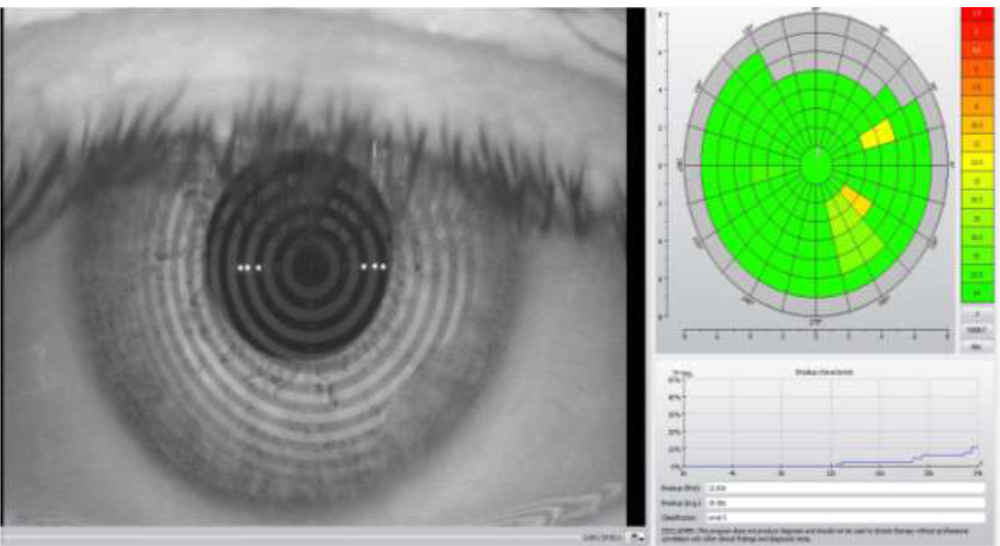
The time requiredfor the tear film to break up following a blink is calledTear Break UP Time(TBUT). It is a quantitative test for measurement of tearfilm stability2.We assessed theTBUT by noninvasive method with keratography 5 (Occulus).Its called Non Invasive Keratograph Break Up Time (NIKBUT).It uses a grid or other patterns directed on the precorneal tear film for observation of imagedistortion and time from opening the eyes to the first sign of image distortion is measured in seconds.Placido rings are reflected on the corneal surface. The software analyzes different segments and a distortion in the reflected mires is recorded as a break in the tear film. The results are displayed in a color-coded map, where red/orange segments correspond with a faster break-up time. A break-up characteristics map shows the total area (%) of the cornea affected during the measuring time. The time when the first break in the tear film occurred is displayed, as well as the average time of all the break-ups that occurred during the measurement. The software automatically grades the level .
The normal time for tear film breakup is15–20 seconds and Tear break Up time of less than 10seconds is considered as dry eye (Fig 2 ).TBUT values of less than 5–10 seconds indicate tear instability and are observed in patients with mild to moderate dry eye disease [L. S.Mengher, A. J. Bron, S. R. Tonge, and D. J. Gilbert, “A noninvasive instrument for clinical assessment of the pre-corneal tear film stability,” Current Eye Research, vol. 4, no. 1, pp. 1–7,1985.].
Fig. 2 NIKBUT – Normal eye
NIKBUT – DRYE EYE PATIENT

Tear meniscus Height (TMH) assessment
TMH assessment wasperformed by using the white light acquisition function in keratograph5.TMH measured with a built-in ruler. Generally, TMH is measured in line with the pupil center. Normal TMH > 0.20mm and Irregular TMH can be evaluated along the lid marginFig.3
Fig.3
Tear meniscus height 0.34mm
Tear meniscus height 0.16mm
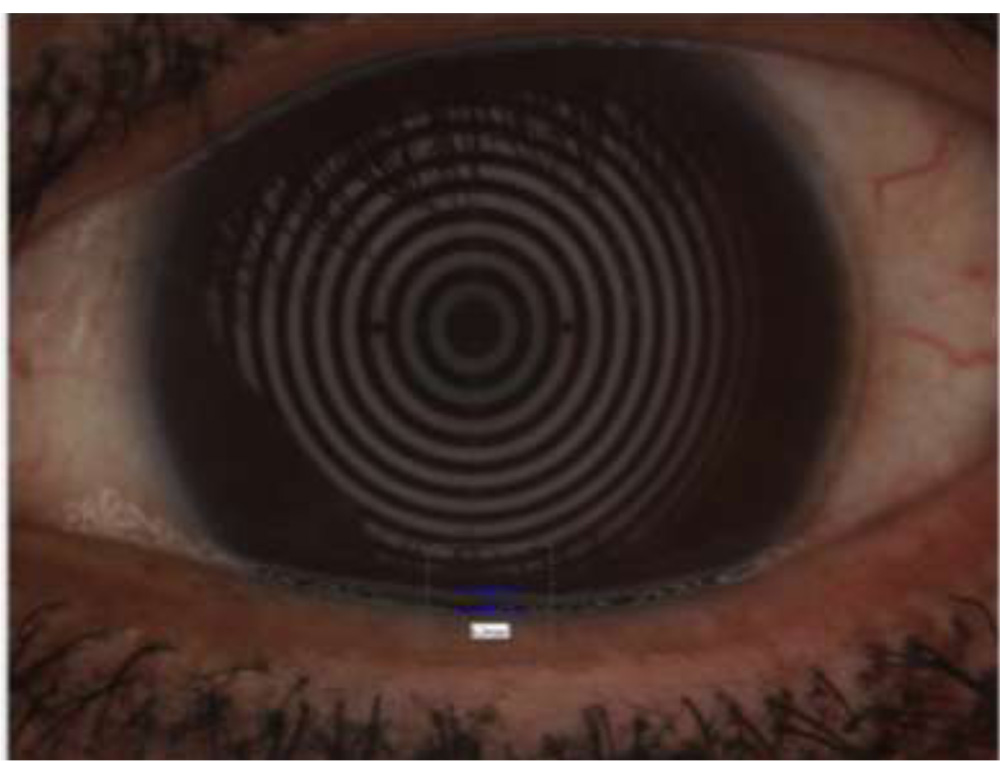
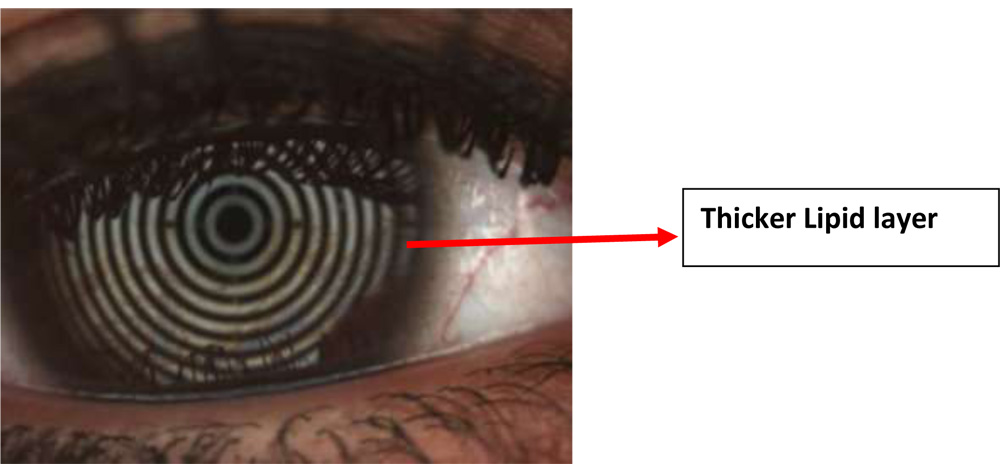
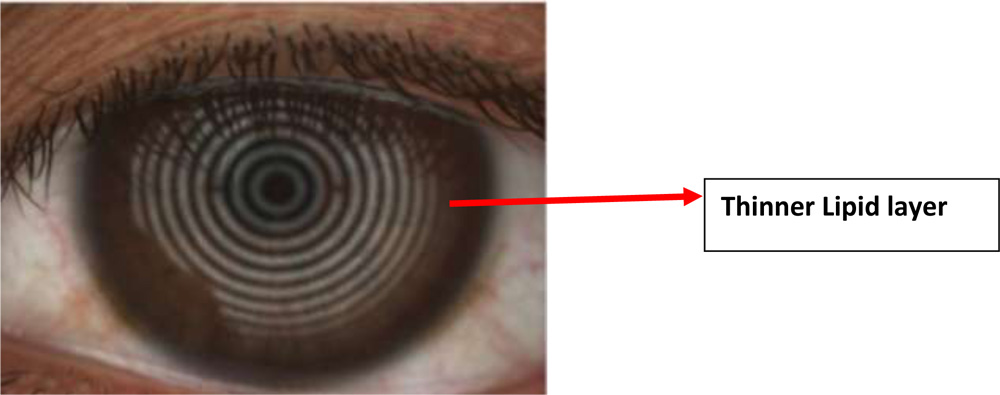
Lipid layer
The quality of Lipid layer was assessed by keratograph5 .The principle of white light interferometry is used while a video or image is recorded.Instructed the patient to blink during recording . Recorded the lipid layer for the duration of two to three eyelid blinks .Thicker lipid layer are indicated by the bronze reflections withLots of colorful fringes .White, colorless reflections can be observed in patients with thin lipid layer.Fig4
Fig.4 Lipid layer showed by Keratograph 5
Assessment of mucin particles in Tear film
Video recording (up to 32 frames per second) performed by the Keratograph 5M is used to observe the distribution of mucinparticles in the tear film (the amount, movement and speed of particles found in the tear film) A fast speed of mucin particles in the tear film after each blink is an indication of a normal tear film. Slow or sluggish movement and increase in the amount of particles seen after the blink is an indication of anirregular or high viscous tear filmFig.5
Fig.5Assessment of mucin particles

Diagnostic tests cut off values has been showed in table 2.
Results
17.07% of the patients who had complaints of dry eye showed negative results in all dry eye studies(fig.6) . Among the rest 83% patients only 19.51% patients were affected by all components and are considered as severe dry eyes; 24.39% had aqueous deficiency; 9.73% lipid deficiency and 7.3% mucin deficiency ;7.3% hyperosmolarity, 9.76% had mucin with aqueous deficiency; 12.24% had lipid with aqueous & 9.73% had lipid with mucin deficiencyFig7. Osmolarity was high in 50% aqueous deficient patients, in 100% lipid deficient & severe dry eye patients.
Aqueous component deficiency was more prevalent and is observed in post LASIK and contact lens wear patients. Fig.8. patients reached menopause and patients with Meibomian gland diseases (MGD)were more prone to had lipid deficiency Fig9.
Fig.6 DRY EYE Vs. NO DRY EYE
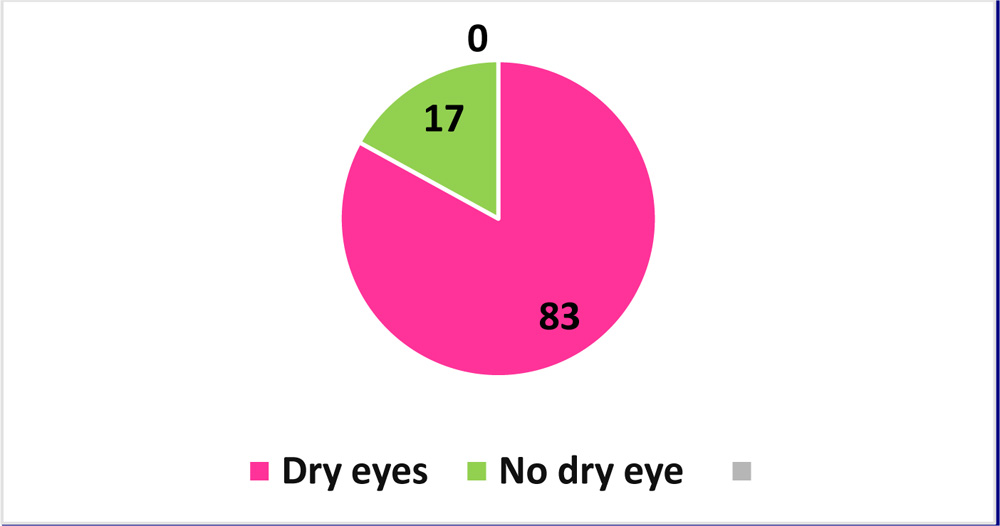
Fig:7Percentage of patients with deficiency of Tear components
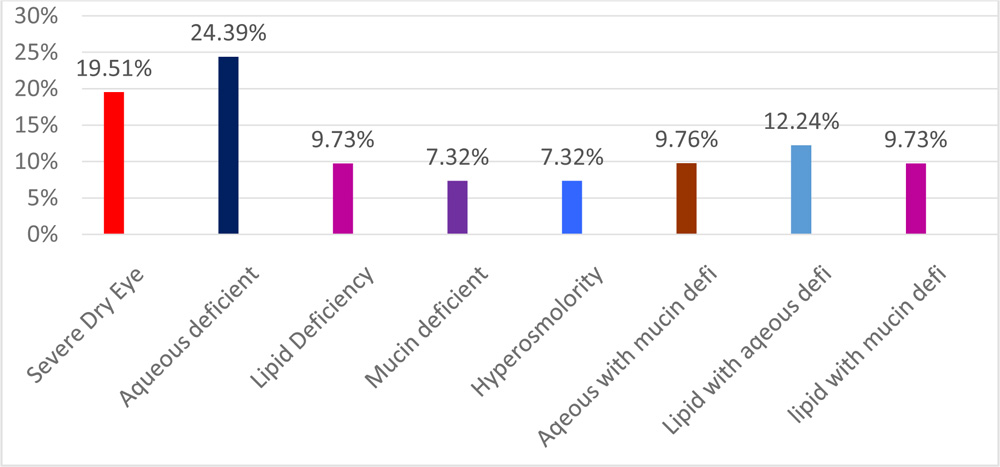
Fig 8 Aqueous deficiency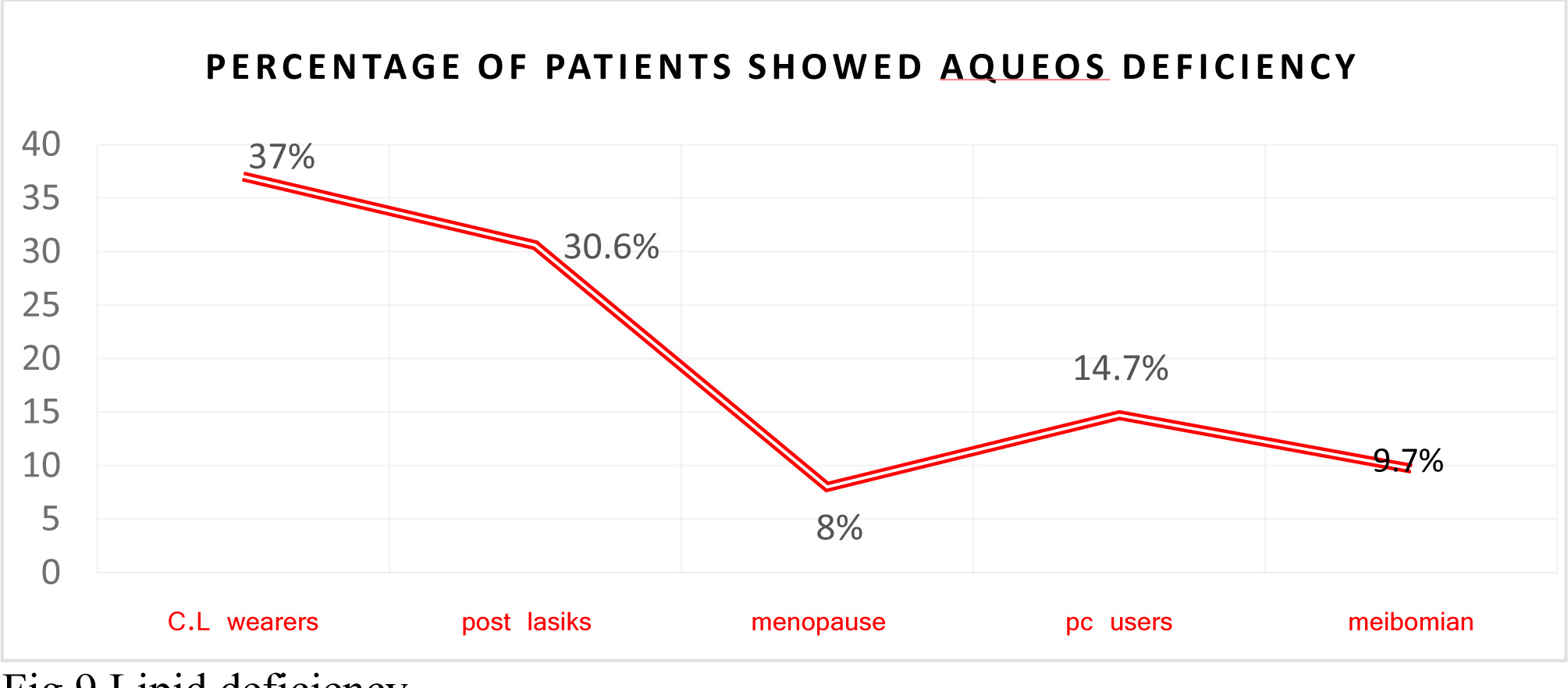
Fig.9 Lipid deficiency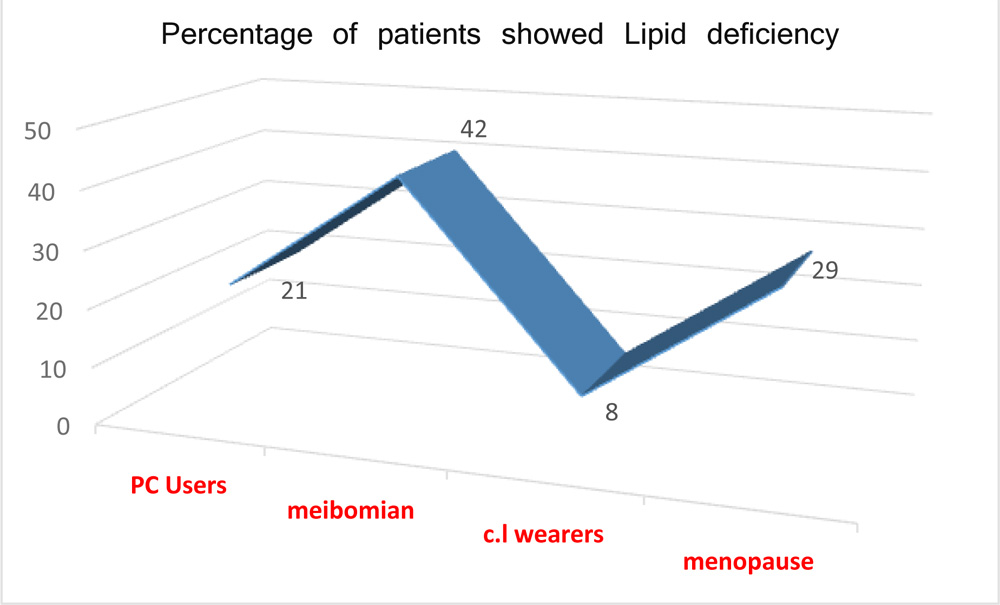
Table2: Diagnostic tests and normal values.
| Test | Normal values |
| Tear film breakup time (TBUT) | >10 sec |
| Noninvasive breakup time (NIBUT) | 15 sec–20 sec |
| Schirmer I test (without topical anesthesia) | >10mm after 3 minutes |
| Tear osmolarity | <290–300mOsm/L |
Discussion
Although it’s a small study, our results showed 17% of patients who had complaint of dry eyes were not really dry eyes. They didn’t show up even a single positive sign of dry eye in any of the tests includedin dry eye work up. Patients were considered as severe dry eye when all the diagnostic tests such as Schirmer test, tear osmolarity , tear meniscus height, lipid layer, mucin layer, tear Break up time showed positive results.Maintenance of a healthy tear film is achieved by a constant feedback mechanism between the ocular surface, brainstem and lacrimal glands, collectively called the Lacrimal Functional Unit.In this study, 24.39% of patients were in the category of aqueous deficient dry eye.Aqueos deficient dry eye is caused by low volume of tear production which results in hyperosmolarity.Our study showed that Contact lens wearers and post Laser assisted in situ keratomileusis (LASIK) surgery patients had significant aqueous deficiency compared to PC users,meibomian Gland dysfunction (MGD) and menopause groups.
Contact lens wear compromises the precorneal film stability and causes the disappearance of the lipid layer in the post-lens fraction which is responsible for the tear film stability. Furthermore this separation of tear film triggers an increase of water evaporation followed by a corresponding increase of the tear osmolarity and consequently resulting in ocular surface damage 30-32. It is hypothesized that mechanisms other than tear film separation, such as changes in corneal epithelium and/or cytokine production, may also contribute to the poorer TBUT and ocular surface disease indicator (OSDI) values in long term wearers.
Dry eye is one of the most common complications of LASIK surgery. Dryness after LASIK has been linked to numerous possible etiologies to include but not limited to, dryness before surgery, female gender and mean spherical equivalent treatment. The most common etiology described is secondary to the transection of corneal nerves and loss of superficial corneal innervation 33-37.These sensory nerves originate from the ophthalmic division of cranial nerve 5, the trigeminal nerve. Classically during flap creation, a superior hinge is created resulting in the greatest transection of corneal nerves since a large proportion of nerves enter from the radial aspects of the cornea. These radial fibers run radially in the middle third of the stroma, divide to form a dense subepithelial plexus and then run perpendicularly to penetrate Bowmans layer and supply the epithelium (Alternating the hinge to the nasal or temporal aspect has been shown to reduce the amount of dryness and lost corneal sensation up to 6 months postoperatively (p < 0.0001) 38However, beyond that time point there are no differences. .In order to possibly decrease dryness caused by flap creation, reducing the flap thickness has been shown to have less of an effect on corneal sensation and tear function tests39
In our study 9.73% had lipid deficiency .Lipids are another component to be taken into account.By means of analysis of lipids intears, it is possible to identify lipids that arealtered in various ocular surface pathologies.Lipids become highly relevant in pathologies such as dry eyeor blepharitis.Disorders of lipid layer are responsible for almost 80% of tear film disorders embraced by the term “dryeye” and are its major etiology 40-41Correspondingly, patients suffering from dry eye exhibit an increased evaporation rate at the eye surface and a higher surface tension of the tear liquid42,43
Results from our study showed that Meibomian gland dysfunction and menopause patients had higher lipid deficiency followed by PC users .Only 8% of contact lens wearers had lipid deficiency .
MGD is hypothesized to occur through the mechanisms of tear film decompensation and evaporative stress from infrequent blinking, which leads to thickening of the oil, blockage of the gland opening and shutdown of oil production in the gland over time which causes the watery layer in the tear film to evaporate. There are many studies reported the high prevalence of MGD IN DRY EYE PATIENTS. To mention a few, Hom et.al reported39% of asymptomatic subjects had MGD 44. Lemp et.al found that 86% of patients with dry eye of known cause had MGD andShimazakiet. al found 65% of eyes with ocular discomfort had MGD45,46
Since women have lower levels of androgens compared to the levels in men, further age-related decreases in androgen levels may diminish the level of androgen amount needed for optimum eye health.47 Along with a decrease in androgen levels, postmenopausal women develop lower levels of estrogen—a hormone that is known to stimulate meibomian glands and help regulate ocular surface homeostasis .48.Together, androgen deficiency and estrogen decrease lead to inadequate lacrimal gland secretion with superimposed tear-film instability in older women and higher risk of developing dry eye.In their study, D.A.Sachaumberg reported the Dry eye prevalence is 9.8% among women aged 75 years or older compared to only 5.7% among women less than 50 years old 49
The analysis of mucins in tears is crucial. Mucins are the glycoproteic component of mucus and their main characteristic is the ability to adhere to hydrophobic as well as hydrophilic molecules. The mucosa layer maintains the lacrimal film adhered to the corneal epithelium, thus avoiding its separation. In addition, it constitutes a barrier against bacterial invasion and inflammatory cells.
Conclusion
17% of patients who came with c/o dry eye didn’t showed dry eye.
Majority of patients who had come with complaints of dry had really dry eye. Aqueous component deficiency was more common and is observed in post LASIK and contact lens wear patients. Menopause and Meibomian gland diseases patients were more prone to have lipid deficiency.
References
- A. Lemp, C. Baudouin, J. Baum et al., “The definition and classification of dry eye disease: report of the definition and classification subcommittee of the international Dry Eye WorkShop,” Ocular Surface, vol. 5, no. 2, pp. 75–92, 2007.
- “Methodologies to diagnose and monitor dry eye disease: report of the diagnostic methodology subcommittee of the international dry eye workshop (2007),”TheOcular Surface, vol.5, no. 2, pp. 108–152, 2007.
- Uchino, Y. Uchino, M. Dogru et al., “Dry eye disease and work productivity loss in visual display users: the Osaka study,” The American Journal of Ophthalmology, vol. 157, no. 2, pp. 294– 300, 2014.
- R. Grubbs Jr., S. Tolleson-Rinehart, K. Huynh, and R. M. Davis, “A review of quality of life measures in dry eye questionnaires,” Cornea, vol. 33, no. 2, pp. 215–218, 2014.
- Paulsen, K. J. Cruickshanks,M. E. Fischer et al., “Dry eye in the beaver dam offspring study: prevalence, risk factors, and health-related quality of life,” American Journal of Ophthalmology, vol. 157, no. 4, pp. 799–806, 2014.
- Miljanovi´c, R. Dana, D. A. Sullivan, and D. A. Schaumberg, “Impact of dry eye syndrome on vision-related quality of life,” American Journal of Ophthalmology, vol. 143, no. 3, pp. 409.e2– 415.e2, 2007.
- Tong, S. Waduthantri, T. Y. Wong et al., “Impact of symptomatic dry eye on vision-related daily activities: the Singapore malay eye study,” Eye, vol. 24, no. 9, pp. 1486–1491, 2010.
- Mishima S, Gasset A, Klyce S, B aum J. Determination of tear v olumeandtear Investigativ e Op h thalm o lo g y 1966; 5: 264-76.
- ScherzW ,Dohlman CH. Is the lacrimal gland dispensable? keratoconjunctivitissicca after lacrimal gland remov al. Arch Op h thalm o l 1975;93: 81-3.
- Li DQ, Chen Z , Song X J, et al. Stimulation of matrix metalloproteinases by hyperosmolarity via a JNK p athway in human corneal epithelial cells. Invest Op h thalmol Vis Sci 2004;45:4302-11 57.
- Luo L, Li DQ, Corrales RM, P ugfelder SC. Hyperosmolar saline is a proinflamatory stress on the mouse ocular surface. E ye Contact Lens 2005;31:186-93.
- De Paiv a CS, Corrales RM, Villarreal AL, et al. Corticosteroid and doxycycline sup p ress MMP-9 and in ammatory cytokine expression, MAPK activation in the corneal epithelium in experimental dry eye. ExpE ye Res 2006;83:526-35.
- Mathers WD, Shields WJ, Sachdev MS, PetrollWM,Jester JV. Meibomian gland morphology and tear osmolarity: changes with Accutane therapy.Cornea. 1991; 10: 286-290.
- Gilbard JP, Rossi SR, Heyda KG. Tear film and ocular surface changes after closure of the meibomian gland orifices in the rabbit. Ophthalmology 1989; 96: 1180-1186.
- Lozato PA, Pisella PJ, Baudouin C. Phase lipidique du film lacrymal :physiologie et pathologie. J Fr Ophtalmol 2001; 24: 643-658.
- Tiffany JM. Physiological functions of the meibomian glands. Prog. Retinal Res. 1995; 14: 47-74.
- Diebold Y, Rios JD, Hodges RR, Rawe I, Dartt DA. Presence of nerves and their receptors in mouse and human conjunctival goblet cells. Invest Ophthalmol&VisSci 2001;42:10:2270-2282.
- Watanabe H. Significance of mucin on the ocular surface. Cornea 2002;21:S17-S22.
- Gilbard, JP. Dry-Eye Disorders. In: Albert M, Jakobiec F, Azar D, Gragoudas E, Power S, and Robinson N., eds. Principles and Practice of Ophthalmology: Second Edition, vol. 2. Philadelphia: W.B. Saunders Company, 2000:982-1001.
- Danjo Y, Watanabe H, Tisdale A, Georgoe M, Tsumura T, Abelson M, Gipson I. Alteration of mucin in human conjunctival epithelia in dry eye. Invest Ophthalmol&VisSci 1998;39:13:2602-2609.
- C. Pflugfelder, A. Solomon, andM. E. Stern, “The diagnosis andmanagement of dry eye: a twenty-five-year review,” Cornea, vol. 19, no. 5, pp. 644–649, 2000.
- Yokoi and A. Komuro, “Non-invasive methods of assessing the tear film,” Experimental Eye Research, vol. 78, no. 3, pp. 399–407, 2004.
- Mathers WD. Why the eye becomes dry: a cornea and lacrimal gland feedback model. CLAO J 2000;26:159-65.
- Farris RL, Gilbard JP, Stuchell RN, Mandel ID. Diagnostic tests in keratoconjunctivitissicca. CLAO J 1983;9:23-8.
- Lemp MA. Report of the National Institute/Industry workshop on the clinical trials in dry eyes. CLAO J 1995;21:221-32.
- Gilbard JP, Farris RL, Santamaria J 2nd. Osmolarity of tear microvolumes in keratoconjunctivitissicca. Arch Ophthalmol 1978;96:677-81.
- A. Lemp, A. J. Bron, C. Baudouin et al., “Tear osmolarity in the diagnosis and management of dry eye disease,” The American Journal of Ophthalmology, vol. 151, no. 5, pp. 792–798,2011
- Tomlinson A, Khanal S, Ramaesh K, et al. Tear film osmolarity: determination of a referent for dry eye diagnosis. Invest Ophthalmol Vis Sci. 2006 Oct;47(10):4309-15.
- Doughty MJ: Re-wetting, comfort, lubricant and moistu-rizing solutions for the contact lens wearer. Cont Lens Anterior Eye 1999; 22:116-26.
- Gilbard JP, Gray KL, Rossi SR: A proposed mechanism for increased tear-film osmolarity in contact lens wearers. Am J Ophthalmol 1986; 102:505-7.
- Foulks GN: The correlation between the tear film lipid layer and dry eye disease. SurvOphthalmol 2007; 52:369-74.
- Kastelan S, Lukenda A, Salopek-Rabatić J, Pavan J, Gotovac M: Dry eye symptoms and signs in long-term contact lens wearers. CollAntropol 2013a; 37:199-203.
- Shoja MR, Besharati MR. Dry eye after LASIK for myopia: Incidence and risk factors. European J f Ophthamol 2007; 17:1-6.
- Donnenfeld ED, Solomon K, Perry HD, Doshi SJ, Ehrenhaus M, Solomon R, Biser S. The Effect of hinge position on corneal sensation and dry eye after LASIK. Ophthalmol 2003; 110: 1023-1029.
- Toda I, Asano-Kato N, Komai-Hori Y, Tsubota K. Dry Eye after laser in situ keratomileusis. Am J Ophthamol 2001; 132:1-7.
- DrPaiva CS, Chen Z, Koch DD, Hamill MB, Manual FK, Hassan SS, Wihelmus R, Pflugfelder SC. The incidence and risk factors for developing dry eye after myopic LASIK. Am J Ophthalmol 2006; 141: 438-445.
- Ambrosio R Jr, Tervo T, Wilson SE. LASIK-associated dry eye and neurotrophic epitheliopathy: pathophysiology and strategies for prevention and treatment. J Refract Surg 2008; 4:396-407.
- Barequet IS, Hirsh A, Levinger S. Effect of thin femtosecond LASIK flaps on corneal sensitivity and tear function. J Refract Surg 2008; 24:897-902.
- Golas L, Manche EE. Dry Eye after laser in situ keratomileusis with femtosecond laser and mechanical keratome. J Cataract Refract Surg 2011; 37:1476-80.
- Lemp MA. Report of the National Eye Institute/Industry workshop on Clinical Trials in Dry Eyes. CLAO J. 1995; 21: 221-232.
- Shimazaki J, Sakata M, Tsubota K. Ocular surface changes and discomfort in patients with Meibomian gland dysfunction. Arch Ophthalmol. 1995; 113:1266-1270.
- Golas L, Manche EE. Dry Eye after laser in situ keratomileusis with femtosecond laser and mechanical keratome. J Cataract Refract Surg 2011; 37:1476-80.
- Hom MM, Martinson JR, Knapp LL, Paugh JR. Prevalence of Meibomian gland dysfunction. Optom Vis Sci 1990; 67:710-12
- Lemp MA. Report of the National Eye Institute/Industry workshop on Clinical Trials in Dry Eyes. CLAO J. 1995; 21: 221-232.
- Shimazaki J, Sakata M, Tsubota K. Ocular surface changes and discomfort in patients with Meibomian gland dysfunction. Arch Ophthalmol. 1995; 113:1266-1270.
- Nagyova B, Tiffany JM. Components responsible for the surface tension of human tears. Curr Eye Res. 1999; 19: 4-11
- Zhao J, Manthorpe R, Wollmer P. Surface activity of tear fluid in patients with primary Sjogren’s syndrome. ClinPhysiolFunct Imaging. 2002; 22:24-27.
- Bron AJ, Tomlinson A et. al Rethinking dry eye disease: a perspective on clinical implications Ocul Surf 2014; 12(suppl.2):S1-31.
- Craig JP, Blades K, Patel S. Tear lipid layer structure and stability following expression of the Meibomian glands. Ophthalmic Physiol Opt 1995;15:569-74.
- Hom MM, Martinson JR, Knapp LL, Paugh JR. Prevalence of Meibomian gland dysfunction. Optom Vis Sci 1990; 67:710-12
- Lemp MA, Crews LA, Bron AJ, Foulks GN, Sullivan BD. Distribution of aqueous –deficient and evaporative dry eye in a clinic vased patient cohort: a retrospective study. Cornea 2012;31:472-8.
- Shimazaki J, Sakata M, Tsubota K. Ocular surface changes and discomfort in patients with Meibomian gland dysfunction. Arch ophthalmol 1995;113:1266-70
- Labrie, A. Bélanger, L. Cusan, J. Gomez, and B. Candas, “Marked decline in serum concentrations of adrenal C19 sex steroid precursors and conjugated androgen metabolites during aging,” Journal of Clinical Endocrinology and Metabolism, vol. 82, no. 8, pp. 2396–2402, 1997.
- A. Sullivan, R. V. Jensen, T. Suzuki, and S. M. Richards, “Do sex steroids exert sex-specific and/or opposite effects on gene expression in lacrimal and meibomian glands?” Molecular Vision, vol. 15, pp. 1553–1572, 2009.
- A. Schaumberg, D. A. Sullivan, J. E. Buring, and M. R. Dana, “Prevalence of dry eye syndrome among US women,” American Journal of Ophthalmology, vol. 136, no. 2, pp. 318–326, 2003
- Corrales RM, Narayanan S, Fernández I, Mayo A, Galarreta DJ, et al. Ocular mucin gene expression levels as biomarkers for the diagnosis of dry eye syndrome. Invest Ophthalmol Vis Sci.2011;52:8363–9.
- Salopek-Rabatić J, Pavan J, Kastelan S, Rabatić L: Glaucoma patients and contact lenses-how to fit-how to treat? CollAntropol 2013; 37:195-8.
REFERENCE – DISCUSSION
A.Golas L, Manche EE. Dry Eye after laser in situ keratomileusis with femtosecond laser and mechanical keratome. J Cataract Refract Surg 2011; 37:1476-80.
B.Lemp MA. Report of the National Eye Institute/Industry workshop on Clinical Trials in Dry Eyes. CLAO J. 1995; 21: 221-232.
C.Shimazaki J, Sakata M, Tsubota K. Ocular surface changes and discomfort in patients with Meibomian gland dysfunction. Arch Ophthalmol. 1995; 113:1266-1270.
D.Nagyova B, Tiffany JM. Components responsible for the surface tension of human tears. Curr Eye Res. 1999; 19: 4-11
E.Zhao J, Manthorpe R, Wollmer P. Surface activity of tear fluid in patients with primary Sjogren’s syndrome. ClinPhysiolFunct Imaging. 2002; 22:24-27.
F.Bron AJ, Tomlinson A et. al Rethinking dry eye disease: a perspective on clinical implications Ocul Surf 2014; 12(suppl.2):S1-31.
G.Craig JP, Blades K, Patel S. Tear lipid layer structure and stability following expression of the Meibomian glands. Ophthalmic Physiol Opt 1995;15:569-74.
H.Hom MM, Martinson JR, Knapp LL, Paugh JR. Prevalence of Meibomian gland dysfunction. Optom Vis Sci 1990; 67:710-12
I.Lemp MA, Crews LA, Bron AJ, Foulks GN, Sullivan BD. Distribution of aqueous –deficient and evaporative dry eye in a clinic vased patient cohort: a retrospective study. Cornea 2012;31:472-8.
J.Shimazaki J, Sakata M, Tsubota K. Ocular surface changes and discomfort in patients with Meibomian gland dysfunction. Arch ophthalmol 1995;113:1266-70
K.Labrie, A. Bélanger, L. Cusan, J. Gomez, and B. Candas, “Marked decline in serum concentrations of adrenal C19 sex steroid precursors and conjugated androgen metabolites during aging,” Journal of Clinical Endocrinology and Metabolism, vol. 82, no. 8, pp. 2396–2402, 1997.
L.A. Sullivan, R. V. Jensen, T. Suzuki, and S. M. Richards, “Do sex steroids exert sex-specific and/or opposite effects on gene expression in lacrimal and meibomian glands?” Molecular Vision, vol. 15, pp. 1553–1572, 2009.
M.A. Schaumberg, D. A. Sullivan, J. E. Buring, and M. R. Dana, “Prevalence of dry eye syndrome among US women,” American Journal of Ophthalmology, vol. 136, no. 2, pp. 318–326, 2003
N.Corrales RM, Narayanan S, Fernández I, Mayo A, Galarreta DJ, et al. Ocular mucin gene expression levels as biomarkers for the diagnosis of dry eye syndrome. Invest Ophthalmol Vis Sci.2011;52:8363–9.
O.Salopek-Rabatić J, Pavan J, Kastelan S, Rabatić L: Glaucoma patients and contact lenses-how to fit-how to treat? CollAntropol 2013; 37:195-8.