 FP752 : Outcomes of a Management Strategy in Eyes with Corneal Irregularity and Cataract.
FP752 : Outcomes of a Management Strategy in Eyes with Corneal Irregularity and Cataract.![]()
AIOS – Sante Vision Award
Dr. Tejal S. J. T16491, Dr. Mathew Kurian, Dr. Rohit Shetty, Dr. Luci Kaweri
Abstract
- Abstract
- Purpose: To evaluate the outcomes of a management strategy in patients with irregular corneas and cataract.
- Methods: Six eyes of four patients presented for cataract surgery with irregular corneas following corneal refractive surgery. Topo-guided ablation regularized the cornea, followed by phacoemulsification and intraocular lens implantation. Zonal keratometric coefficient of variation (ZKCV) measured structural changes and visual quality metrics measured functional
- Results: The mean duration after corneal refractive surgery was 7.83 ± 2.40 years. The logmar uncorrected distance visual acuity (0.67±0.25) and the corrected distance visual acuity (0.38 ±0.20) improved to 0.34±0.14 and 0.18±0.10 respectively. The changes in the standard deviations of the zonal keratometry values and the ZKCV were statistically significant in the 2, 3 and 4 mm zones. The changes in the Strehl ratio (ANOVA p=0.043) was also statistically significant.
- Conclusions: Corneal regularization followed by phacoemulsification resulted in lower residual refractive error with improved visual quality metrics. This strategy is a viable option in patients with symptomatic cataracts and irregular corneas.
INTRODUCTION
- INTRODUCTION
- Since its birth 25 years back, laser assisted in-situ keratomileusis (LASIK) has been using exciter laser ablation to reshape the cornea and correct refractive error[1] Those patients who underwent LASIK in early days, are now presenting with age-related cataracts. Surgeries done in early years when the nomogram was being revised, had resulted in few cases of irregular corneas.
- Small or decentred optical zones, irregular ablations and central islands are associated with high corneal higher order aberrations (HOAs).[2,3] Obtaining optimal optical outcomes with cataract surgery in such cases is difficult. The dilemma of regularizing the cornea first followed by cataract surgery or vice-versa is also unresolved.
- Topography guided Customised Ablation Treatment (T-CAT) outcomes improve visual acuity and quality in irregular corneas.[4] Refractive surgery complications, such as post-LASIK ectasia, decentered ablation, small optical zones, have been successfully treated with this modality.[5] We hereby describe a method of customising the cataract surgeries in irregular corneas by doing a topo-guided ablation to reduce corneal irregularity, assessing stability of keratometry and irregularity, followed by cataract surgery.
METHODS
- METHODS
- This was a prospective interventional case series adhering to the tenets of the Declaration of Helsinki with institutional ethical board clearance. Patients presenting with symptomatic cataracts and history of laser in situ keratomileusis (LASIK) in the same eye and giving informed consent were included.
- Exclusion criteria included pre-existing ocular or chronic systemic disease, pregnant or nursing women and one-eyed patients. All patients underwent refraction, slit-lamp examination, indirect ophthalmoscopy and topography using the Pentacam HR (Oculus Optikgeräte GmbH). Axial length measurements were by immersion biometry when optical biometry was not possible.
- Eyes with post LASIK corneal irregularities, no evidence of ectasia on Pentacam HR and with minimal corneal pachymetry of 400 microns, underwent corneal regularisation using the topography-guided customized ablation treatment (T-CAT) software linked with the Allegretto Topolyzer system (WaveLight Laser Technologie AG, Germany). Adjunct corneal collagen crosslinking was not planned for this study subset patients as the predicted minimum pachymetrywas more than 380 microns in all cases. An average of eight maps with at least 90% data was taken by Allegretto topolyzer system. The optical zone diameter was restricted to 5.5 – 6.0 mm after defining the target asphericity (Q-value) within a range 0 to -0.6. Under topical anaesthesia(proparacaine 0.5%; Alcon Inc.,Fort Worth USA), the pre existing flap was raised, the planned laser ablation was performed, followed by balanced salt solution irrigation of the residual stromal bed. Post-operative regime was prednisolone acetate 1% (Pred Forte® prednisolone acetate ophthalmic suspension, Allergan, India) eye drops four times daily tapered weekly, moxifloxacin 5% eye drops (Vigamox®, Alcon Inc., Fort Worth, USA) four times daily for one week with lubricating eye drops (Optive®, Allergan, India) four times daily.
- The IOL power was calculated after achieving keratometric stability defined as change of 0.2 dioptre or less in standard deviation of mean K over three consecutive visits. The IOL power chosen for implantation was the minimum IOL power obtained on American Society of Cataract and Refractive Surgery (ASCRS) post LASIK calculator.[6] Patients underwent phacoemulsification by a single surgeon (MKK) using a temporal clear corneal incision. AssessmentsThe Holladay’s equivalent keratometry reading (EKR) map on the Pentacam presents the mean equivalent keratometry readings and their standard deviations in zones around the corneal apex. We derived the Zonal Keratometric Coefficient of Variation (ZKCV) (dispersion of data points in a data series around the mean) from the zonal standard deviation and the zonal Mean Keratometry as follows:ZKCV= zonal keratometric standard deviation / zonal Mean Keratometry x 100Efficacy assessments were the improvement in structural and functional parameters and safety was the percentage of eyes with loss of two or more lines of CDVA.[7]
- Statistical Analysis
- SPSS version 17 was used for statistical analysis. The Shapiro-Wilk test checked normal distribution of continuous variables. Comparisons between groups were 2-sided to a significance of 0.05.
RESULTS
This study included six eyes, three right and three left of four patients, one male and three females, with a mean age of 41.25 ± 9.95 years. The mean duration after LASIK was 7.83 ± 2.40 years while the mean duration between T-CAT and cataract surgery was 1.5 months. The logmar uncorrected distance visual acuity (UDVA) at the time of presentation was 0.67 ± 0.25 (95%CI 0.404 to 0.929) and following TPRK and cataract surgery showed a statistically significant improvement (Paired Samples Test p=0.006) to 0.35 ± 0.14 (95% CI 0.205 to 0.495). The corrected distance visual acuity (CDVA) improvement from 0.38 ± 0.20 (95%CI 0.169 to 0.598) to 0.18 ± 0.10 (95%CI 0.080 to 0.287) was not statistically significant (Wilcoxon Signed Ranks Test p=0.066).
The mean thinning in pachymetry after TCAT was 33 ± 16 microns at pupillary centre, 36 ± 17 microns at apex and 32 ±17 microns at the thinnest corneal thickness on Pentacam HR. Predicted Minimum pachymetry after treatment was 407 ± 16 microns with thinnest pachymetrybeing 380 microns. The RMS difference in the mean K showed a change of 2.12 D in the 1mm zone and 1.40D in the 4 mm zone. The mean reduction in the astigmatism (EKR 65% astigmatism) and the standard deviations of the K values were statistically significant from the 2mm to 4mm zone. The ZKCV showed a statistically significant reduction in the dispersion of measured keratometric data points around the mean keratometry for the 1 and 2 mm zones (Table 1). The changes in the Strehl ratio (ANOVA p=0.043) was statistically significant while the change in mean HOAs (Friedman test p=0.115) and area under the curve of the MTF curve (ANOVA p=0. 356) was not.
The mean IOL power used was 15.25 ± 3.52 D. In four of six (66%) eyes where the IOL power could be calculated pre and post T-CAT the root mean square (RMS) change in the ASCRS calculator minimum IOL power was 0.63D and in the maximum IOL power was 1.30D. The procedure was 100% safe as none of the eyes had loss of two or more lines of vision. Two of six patients were within 0.5 dioptre sphere (DS) and four of six patients were within 1 DS.
RESULTS
This study included six eyes, three right and three left of four patients, one male and three females, with a mean age of 41.25 ± 9.95 years. The mean duration after LASIK was 7.83 ± 2.40 years while the mean duration between T-CAT and cataract surgery was 1.5 months. The logmar uncorrected distance visual acuity (UDVA) at the time of presentation was 0.67 ± 0.25 (95%CI 0.404 to 0.929) and following TPRK and cataract surgery showed a statistically significant improvement (Paired Samples Test p=0.006) to 0.35 ± 0.14 (95% CI 0.205 to 0.495). The corrected distance visual acuity (CDVA) improvement from 0.38 ± 0.20 (95%CI 0.169 to 0.598) to 0.18 ± 0.10 (95%CI 0.080 to 0.287) was not statistically significant (Wilcoxon Signed Ranks Test p=0.066).
The mean thinning in pachymetry after TCAT was 33 ± 16 microns at pupillary centre, 36 ± 17 microns at apex and 32 ±17 microns at the thinnest corneal thickness on Pentacam HR. Predicted Minimum pachymetry after treatment was 407 ± 16 microns with thinnest pachymetry being 380 microns. The RMS difference in the mean K showed a change of 2.12 D in the 1mm zone and 1.40D in the 4 mm zone. The mean reduction in the astigmatism (EKR 65% astigmatism) and the standard deviations of the K values were statistically significant from the 2mm to 4mm zone. The ZKCV showed a statistically significant reduction in the dispersion of measured keratometric data points around the mean keratometry for the 1 and 2 mm zones (Table 1). The changes in the Strehl ratio (ANOVA p=0.043) was statistically significant while the change in mean HOAs (Friedman test p=0.115) and area under the curve of the MTF curve (ANOVA p=0. 356) was not.
The mean IOL power used was 15.25 ± 3.52 D. In four of six (66%) eyes where the IOL power could be calculated pre and post T-CAT the root mean square (RMS) change in the ASCRS calculator minimum IOL power was 0.63D and in the maximum IOL power was 1.30D. The procedure was 100% safe as none of the eyes had loss of two or more lines of vision. Two of six patients were within 0.5 dioptre sphere (DS) and fournof six patients were within 1 DS.
DISCUSSION
Patients with myopic LASIK present with cataracts early as compared to general population.[8] Similar to the study done by Iijima K et al, our patients presented with cataract at an average age of 42 years. Incidence of post-LASIK cataract is low, almost 1 in 100 cases of normal cataracts.[8] Those with irregular astigmatism post LASIK and cataract is even rare and to the best of our knowledge no study has reported the management strategy in such cases.
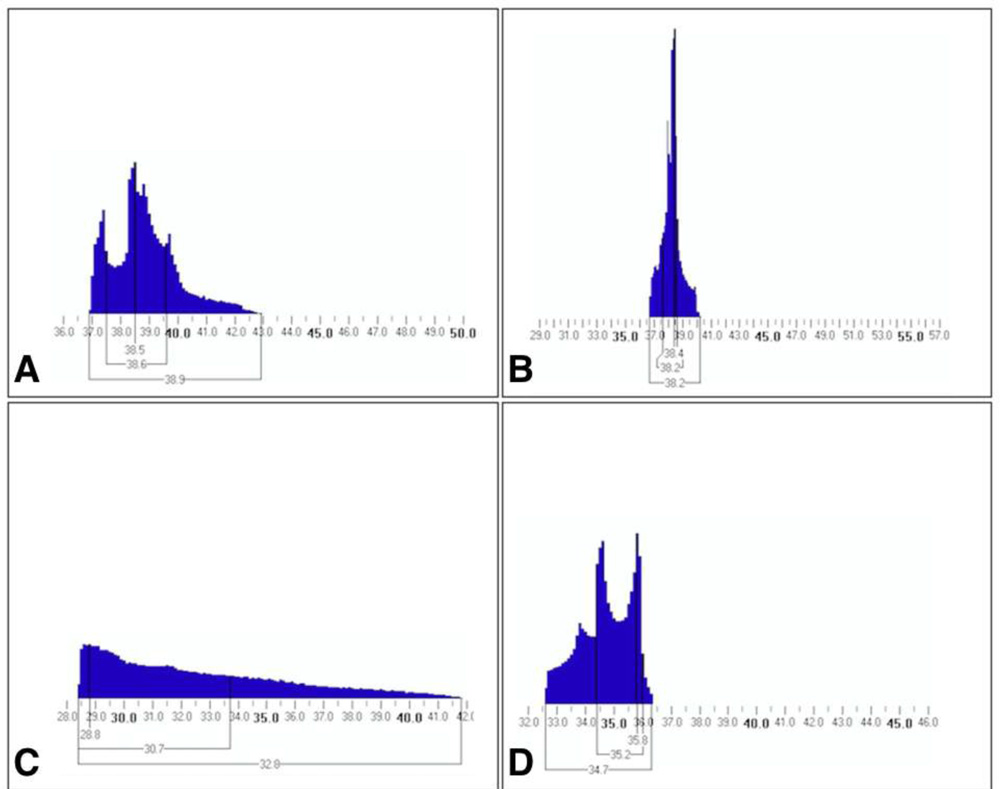
Topographically irregular astigmatism has been classified as regularly irregular (asymmetric bow-tie or angled bow-tie or non orthogonal astigmatism) and irregularly irregular (no recognizable pattern).[9] Irregular astigmatism after LASIK depends on the amount of surgery the eye received, the time since surgery, the size and centration of the optical zone and the occurrence of any intraoperative complications.[10] Irregularity is measured by assessing Zernike HOAs or Fourier irregularity whichdo not give a measure of the variability of the keratometrywith it. Therefore a cataract surgeon has to estimate the impact of the pre-existing corneal irregularity on the mean keratometry values needed for IOL power calculation. We describe a novel method of quantifying the corneal irregularity from the detailed Holladay Report by assessing the mean zonal keratometric coefficient of variation. We analysed the values only uptothe 4 mm zone assuming that as the mesopic pupil diameter. Because of its unique therapeutic benefits in treatment of highly irregular corneas, TCAT was our treatment of choice.[11] All our patients showed improved regularity of cornea after T-CAT as there was 45% reduction in astigmatism, 52% reduction in standard deviation of K values and 51% in ZKCV till the 4mm zone and this improvement was reflected in the improved EKR histogram (FIGURE 1). Following stabilization of keratometry, cataract surgery was performed with IOL implant power selected using the online ASCRS calculator targeting emmetropia.[12] In eyes with a central island T-CAT would result in a relatively steeper central cornea resulting in a myopic shift in IOL power requirement and in eyes with decentred ablations T-CAT would result in relative central flattening cornea resulting in a hyperpic shift in IOL power requirement
(FIGURE 2)
- Our study is limited by its small sample size and no randomized comparison group. We also limited the duration post TCAT to average 6 weeks because of the need for early visual rehabilitation. Possibility of corneal remodelling for longer duration persists. In absence of standard guidelines, we waited for 3 consecutive follow ups showing stability in terms of mean K fluctuation. Conventionally, a secondary LASIK or surface ablation has been the procedure of choice for post cataract refractive surprises.[13] However, the alteration in the mean keratometry values by the TCAT would induce an unpredictable myopic or hyperopic shift in refraction depending on the nature of pre-existing irregularity and treatment plan. Our strategy of treating the cornea by TCAT first followed by cataract surgery is a safe and effective way of optimising results in these cases. It is a relatively rare situation case series and also case series to propose a novel sequence of performing the procedures.
- Numbers are bound to increase with time as more of the baby boomers/early LASIK patients and those with complications will require cataract surgery. So we are putting the results for peer review and will expand the study to a case control / randomised control trial (RCT). If this strategy is seen to work in RCT / case control trial then can consider as an option for irregular astigmatism of all etiologies with cataract.
References:
- Sakimoto T, Rosenblatt MI, Azar DT. Laser eye surgery for refractive errors. Lancet. 2006 Apr 29;367(9520):1432-47. Review
- Mrochen M, Kaemmerer M, Mierdel P, Seiler T. Increased higher-order optical aberrations after laser refractive surgery: a problem of subclinical decentration. J Cataract Refract Surg2001;27:362–369.
- McCormick GJ, Porter J, Cox IG, MacRae S, Higher-Order Aberrations in Eyes with Irregular Corneas after Laser Refractive Surgery. Ophthalmology. 2005 Oct; 112(10):1699-709.
- Mrochen M, Krueger RR, Bueeler M, Seiler T. Aberration-sensing and wavefront-guided laser in situ keratomileusis: management of decentered ablation. J Refract Surg. 2002; 18:418-429.
- Holland S, Lin DT, Tan JC. Topography-guided laser refractive surgery. CurrOpin Ophthalmol.2013 Jul;24(4):302-9.
- Yang R, Yeh A, George MR, Rahman M, Boerman H, Wang M. Comparison of intraocular lens power calculation methods after myopic laser refractive surgery without previous refractive surgery data. J Cataract Refract Surg. 2013 Sep;39(9):1327-35.
- Reinstein DZ, Waring GO 3rd. Graphic reporting of outcomes of refractive surgery. J Refract Surg. 2009 Nov;25(11):975-8.
- Iijima K, Kamiya K, Shimizu K, Igarashi A, Komatsu M. Demographics of patients having cataract surgery after laser in situ keratomileusis. J Cataract Refract Surg. 2015 Feb;41(2):334-8.
- Goggin M, Alpins N, Schmid LM. Management of irregular astigmatism.CurrOpin Ophthalmol.2000 Aug;11(4):260-6. Review.
- Baek TM, Lee KH, Tomidokoro A, Oshika T. Corneal irregular astigmatism after laser in situ keratomileusis for myopia. Br J Ophthalmol.2001 May;85(5):534-6.
- Pasquali T, Krueger R. Topography-guided laser refractive surgery. CurrOpin Ophthalmol.2012 Jul;23(4):264-8.
12.Yang R, Yeh A, George MR, Rahman M, Boerman H, Wang M. Comparison of intraocular lens power calculation methods after myopic laser refractive surgery without previous refractive surgery data. J Cataract Refract Surg. 2013 Sep;39(9):1327-35.
- Alio JL, Abdelghany AA, Fernández-Buenaga R. Enhancements after cataract surgery. CurrOpinOphthalmol. 2015 Jan;26(1):50-5.
Figure captions:
- FIGURE 1: Equivalent K reading (EKR) histogram to demonstrate the improved outcome following T-CAT. (A) EKR histogram of case 3 is shown pre-operatively with broader baser extending from 37D to 43D with two peaks. (B) Post-operatively the EKR histogram shows a tall peak with a narrow base extending from 37D to less than 40D. (C) The EKR histogram of case 6 is shown pre-operatively with broader base extending from 28.5D to 42D. (D) Post operatively the EKR histogram shows a narrow base from 32.5D to 36.5D with two peaks.
- FIGURE 2: Two eyes with irregular corneas after LASIK. (A) The patient’s cornea shows incomplete ablation with steep areas in the pupillary zone. (B) Intra-operative ablation profile used for treatment during topography-guided customized ablation treatment (T-CAT). (C) Post operatively there is flattening at the center of the cornea in the pupillary zone. D) The patient’s cornea with decentered ablation showing both flat and steep areas in the pupillary zone. E) Intra-operative ablation profile used for treatment during T-CAT. F) Post- operatively there is steepening at the center of the cornea in the pupillary zone.
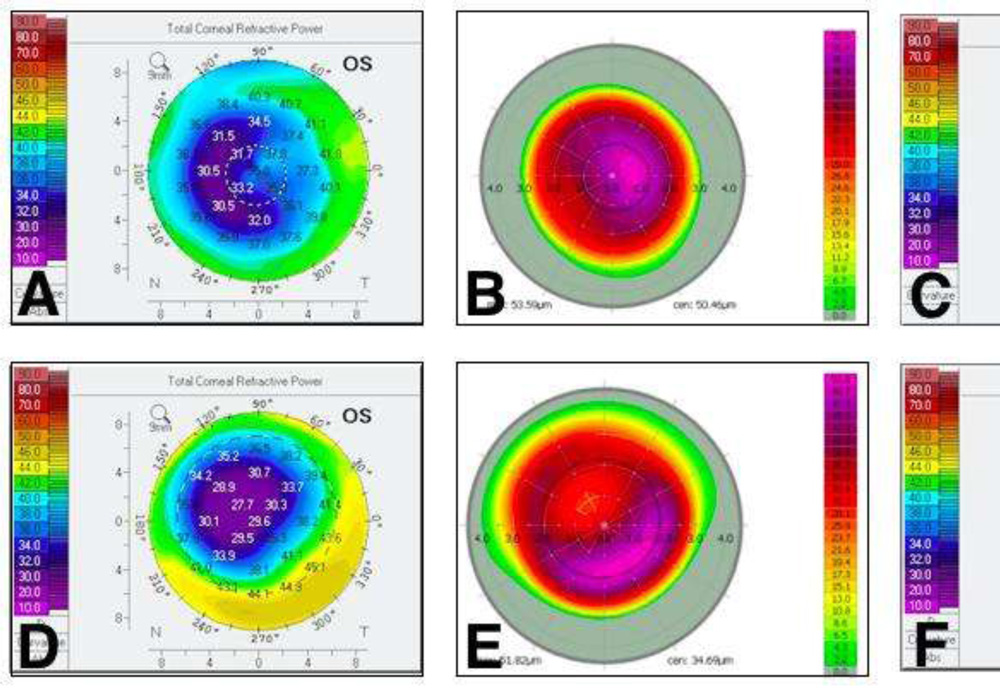
Table 1: Mean ± standard deviation (95% Confidence Interval for Mean) of the baseline variables, post topoguidedcustomised ablation treatment (T-CAT), change from baseline and p- values (paired sample tests) K-Keratometry, EKR 65- Equivalent Keratometry reading in 65% area, SD- Standard deviation,
CV- Coefficient of Variance
| Baseline Mean ± Std. Deviation (95% Confidence Interval for Mean) | Post T-CAT Mean ± Std. Deviation (95% Confidence Interval for Mean) | Change from Baseline | p value (Paired Samples Test) | |
| 1mm mean K | 34.56±4.08 (30.28-38.84) | 34.97±2.94 (31.88-38.06) | 2.12±2.50 | .844 |
| 2mm mean K | 34.33±3.62 (30.53-38.13) | 34.74±2.85 (31.75-37.72) | 1.84±2.27 | . 834 |
| 3mm mean K | 34.61±3.23 (31.23-38.00) | 34.57±2.73 (31.71-37.43) | 1.72+1.65 | .980 |
| 4mm mean K | 34.97±2.67 | 34.55±2.55 | 1.40±1.21 | .791 |
| (32.16-37.77) | (31.87-37.23) | |||
| 1mm Astig EKR65 | 0.93±0.53 (0.37-1.49) | 0.47±0.44 (0.01-0.93) | 0.55±0.51 | .133 |
| 2mm Astig EKR65 | 1.40±0.37 (1.01-1.79) | 0.62±0.42 (0.30-1.07) | 0.82±0.37 | .007 |
| 3mm Astig EKR65 | 1.41±0.43 (0.95-1.86) | 0.59±0.30 (0.27-0.90) | 0.82±0.45 | .003 |
| 4mm Astig EKR65 | 1.48±0.41 (1.05-1.91) | 0.67±0.30 (0.35-0.98) | 0.81±0.47 | .003 |
| 1mm SD | 0.84±0.44 (0.38-1.30) | 0.42±0.14 (0.27-0.57) | 0.46±0.44 | .051 |
| 2mm SD | 1.28±0.54 (0.71-1.84) | 0.71±0.24 (0.45-0.96) | 0.58±0.46 | .040 |
| 3mm SD | 1.66±0.76 (0.86-2.46) | 0.87±0.29 (0.57-1.17) | 0.79±0.62 | .038 |
| 4mm SD | 2.03±0.97 (1.01-3.0) | 0.99±0.38 (0.59-1.39) | 1.04±0.77 | .035 |
| 1mm CV | 2.45±1.24 (1.14-3.75) | 1.21±0.40 (0.79-1.63) | 1.36±1.27 | .042 |
| 2mm CV | 3.84±1.76 (2.00-5.69) | 2.06±0.79 (1.23-2.88) | 1.81±1.57 | .047 |
| 3mm CV | 4.98±2.58 (2.28-7.68) | 2.56±1.03 (1.48-3.64) | 2.42±2.16 | .058 |
| 4mm CV | 5.99±3.19 (2.64-9.33) | 2.94±1.34 (1.53-4.35) | 3.05±2.56 | .056 |