Dr. Apoorva A G, A15802, Dr.Mithila Rajendra, Dr. Shrinivas M Joshi, Dr.Guruprasad Ayachit
Synopsis – To analyse indications,complications and outcomes of retro-fixated iris claw lens and scleral fixated lens. Retrospective analysis of records of ICIOL(n=100) and SFIOL(n=100)( Jan 15- Dec 15) was carried out. Most common indication was subluxated lens (ICIOL-38%,SFIOL-31%)Mean post op BCVA better in SFIOL(0.51) than ICIOL(0.68)(p- 0.016).Iris claw group had higher incidence of PPV + frag compared to SFIOL(p-0.048).Vitreous in AC(p-0.043), hypotony(0.01) and pupil ovalisation(<0.001) were seen more in ICIOL than SFIOL.11% in Iris claw group underwent re-surgery (2% in SFIOL,p-0.01)Results show that although ICIOL has lesser surgical time, SFIOL is a better option due to fewer re surgeries, lesser complication rate and better visual outcomes.
Introduction– Anterior chamber IOLs and scleral-fixated PC IOLs have been popular types of IOLs used in implantation in the absence of adequate capsule support. However, there is much discussion on the bestmethod for secondary IOL implantation that offers the lowest complication rate and best possible visual rehabilitation over several years. Scleral fixated IOLs have withstood the test of time, but at the same time are time consuming procedures and need considerable expertise. Retro-pupillary fixation of an iris-claw IOL has the advantages of true posterior chamber implantation, which results in a deeper anterior chamber and greater distance to the corneal endothelium and has a lower intraoperative and postoperative risk profile.1The purpose of this study was to study and compare the indications, results and complications of ICIOLs and SFIOLs in the setting of poor/no capsular support.
Materials and methods– Restrospective chart review was done of 200 patients who underwent either retro-fixated Iris Claw or Scleral fixated Lens at M M Joshi Eye Institute, Hubli. (January 2015 – December 2015). They were divided into Iris- claw group (Group I) (n=100) and Scleral- fixated IOL group (Group S) (n=100). The Pre-op BCVA, Anterior segment findings on Slit lamp, IOP, posterior segment findings and indications for surgery were noted. Mean follow up was 6 months.
Surgery in group I was done under peri-bulbar anaesthesia. A superior fornix-based Conjunctival peritomy was done. A 6.5 mmcorneo-scleral incision was made in cases where it was not present. Additional procedures viz. anterior vitrectomy or fragmentations if done were recorded. The Iris Claw lens was held with a special iris claw holding forceps and introduced in the AC under OVD. Using a Dialler from a side port, the Iris- claw lens was enclaved to the posterior iris surface. The lens was thus fixed to the mid-peripheral, immobile and less vascular part of the iris. Lens was then released after ensuring its stability. Wound was closed using a 10-0 nylon suture.
 Fig 1- Iris Claw lens being enclaved using a Sinskey hook
Fig 1- Iris Claw lens being enclaved using a Sinskey hook
In group S, surgery was done under peri-bulbar anaesthesia. 270 degree conjunctival peritomy was done. A 6.5 mmcorneo- scleral tunnel was made. Two partial thickness scleral flaps were made 1 mm from the limbus, at 3 and 9 o clock positions. A 9-0 prolene suture was passed from underneath the flap on one side, docked to a 26 Gauge needle, and brought out from under the scleral flap on the opposite side. The suture was then pulled out through the main wound and tied to the eyelets of the haptics of the SFIOL. The sutures were then tied on each side to the bed of the scleral flaps. Additional intra operative manoeuvres and operating time were noted as in group I.
Post operative complications like corneal edema, AC cells, hypotony, striate keratopathy, IOL decentration, instability, disenclavation, pupil ovalisation, CME, Vitreous haemorrhage, RD and so on were noted.
The numbers of re-surgeries needed were also noted in both groups.
Results– 200 patient charts were reviewed. Both groups were equally matched with respect to the side of the eye. The indications for surgery were able to be divided broadly into Intraoperative PCR, surgical aphakia, cataract surgery complications like nucleus drop and dislocated IOL; subluxatedcataract, zonular dialysis and others. The others group comprised of 4 patients, 2 of which were cases with pseudoexfoliation with posteriorly dislocated lens, 1 was a silicon filled eye for secondary IOL implantation, another was a refractive surprise post cataract surgery. In both groups, subluxatedcataract was the commonest indication (Group I- 28%; Group S- 31%). The second commonest etiology was intraoperative posterior capsule rupture (group I- 18%, Group S- 15%)
Pre-operative vision in both groups was comparable. Group I had pre-op vision (log Mar Mean ±SD) 1.99±0.75 and Group S had 1.70 ±0.68 (p value 0.77). There was no significant difference in IOP between two groups Pre op. (Group I 14.9± 9.5; Group S 13.1±5.3; p value 0.80)
A note of additional intra operative procedures was done. Anterior vitrectomy was found to be the most common manoeuvre (42% in Group I and 50% in Group S). Par plana Vitrectomy + fragmentation (PPV+frag) of dropped nucleus or nucleus fragments was done in 20% of Group I and 10% in group S. Other additional manoeuvres performed were Pupilloplasty (more in the SFIOL group,n=11, p value-0.01) ; IOL explantation, Silicon oil removal, and Trabeculectomy. In the study significant difference was observed in additional surgeries required among both groups. Iris claw group required PPV + frag(p value 0.048) higher than in SFIOL group.Pupilloplasty was required in SFIOL group significantly higher than Iris claw group.
| Group | P value | |||||
| Iris Claw | SFIOL | |||||
| Count | % | Count | % | |||
| Anterior vitrectomy | 42 | 42.0% | 50 | 50.0% | 0.256 | |
| PPV+ Frag | 20 | 20.0% | 10 | 10.0% | 0.048* | |
| IOL explantation | 9 | 9.0% | 9 | 9.0% | 1.000 | |
| Trabeculectomy | 6 | 6.0% | 1 | 1.0% | 0.054 | |
| Pupilloplasty | 2 | 2.0% | 11 | 11.0% | 0.01* | |
| SOR | 3 | 3.0% | 2 | 2.0% | 0.651 | |
Table 1
Complications- Striate keratopathy and Pupil ovalisation were the most common complications among Iris claw group. In SFIOL group,striate keratopathy and Uveitis were the most common complications. Vitreous in Anterior chamber (Group I n=4, Group S n=0) (p value 0.043), hypotony (Group I n=11, Group S n=2) and pupil ovalisation (Group I n=37, Group S n=2) were thus significantly higher in the Iris claw group. There were other complications seen in both groups such as disenclavation (subluxation in cases of SFIOL), Vitreous haemorrhage, cystoid macular edema but the difference between the two groups was not significant. Retinal detachment was seen in 3 eyes that underwent SFIOL.
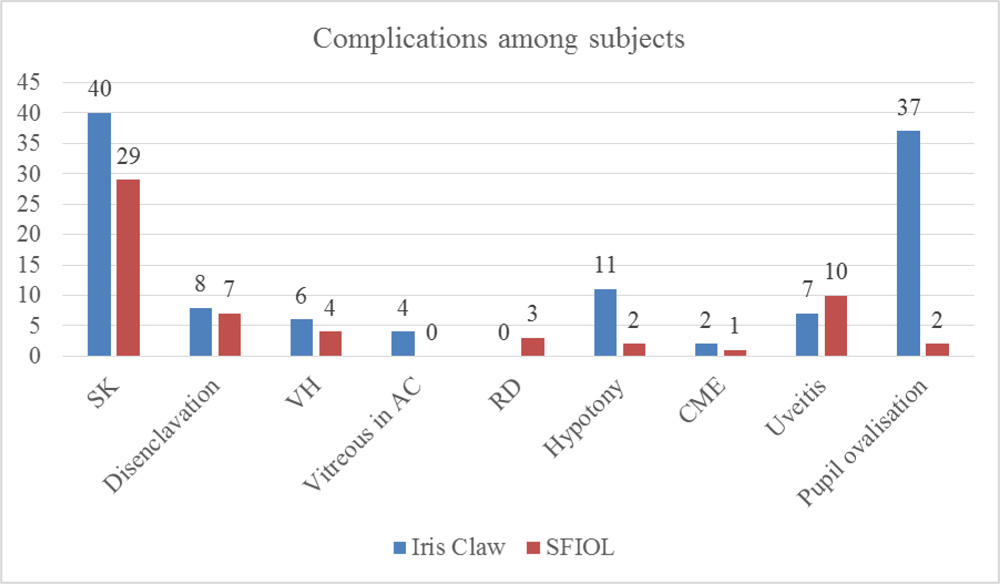 Fig 3- showing the distribution of complications in both groups
Fig 3- showing the distribution of complications in both groups
In the study 11% of subjects in Iris claw underwent re-surgery and 2% in SFIOL group underwent re- surgery. This difference in rate of re- surgery between two groups was statistically significant. Iris claw group underwent tunnel suturing for wound leak in 3 eyes, re-implantation in 1 eye, re-fixation of ICIOL in 5 eyes and Trab+ Mito in 1 eye. SFIOL underwent surgeries for Vitrectomy + membrane surgery + endolaser+ Silicon oil injection for indications unrelated to cataract/ scleral fixation IOL surgery.
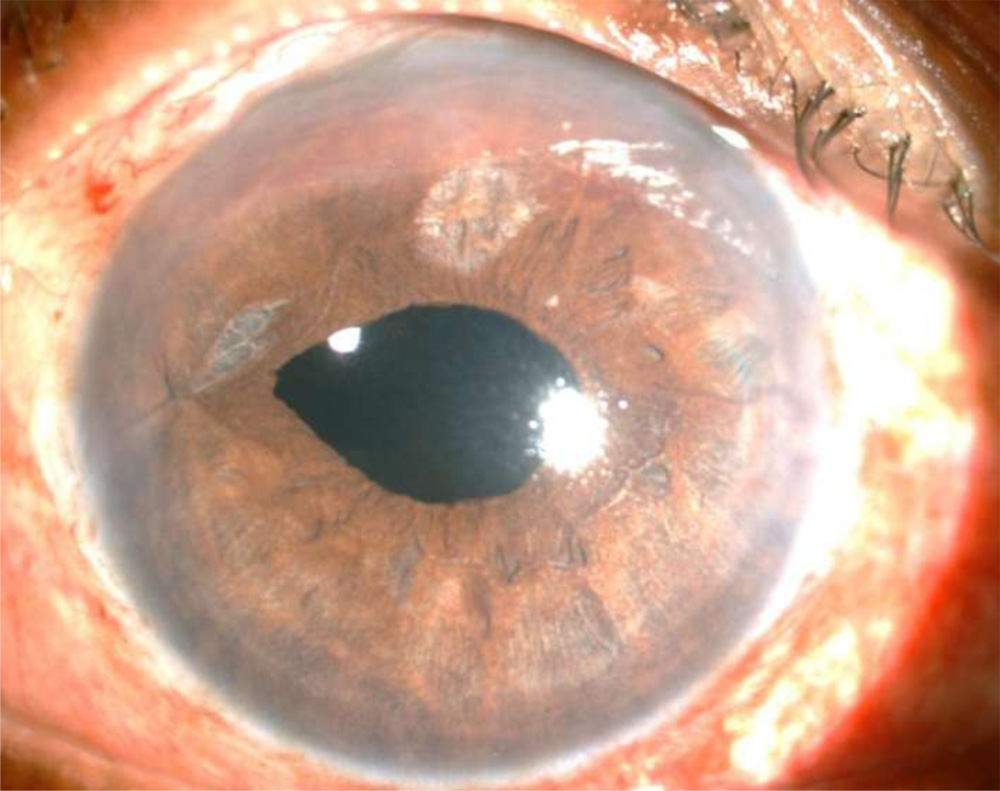 Fig 3- Pupil ovalisation seen with iris chaffing in a case of Iris claw IOL
Fig 3- Pupil ovalisation seen with iris chaffing in a case of Iris claw IOL
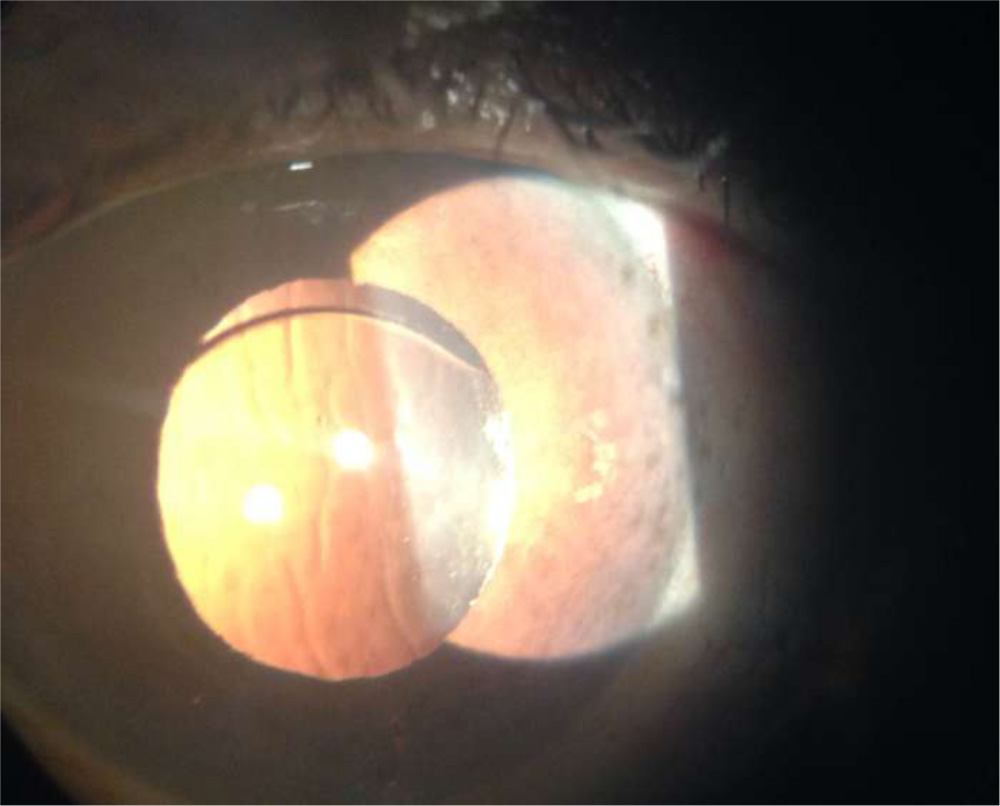 Fig 4- Striae seen on post op day 1 after SFIOL surgery
Fig 4- Striae seen on post op day 1 after SFIOL surgery
Resurgery done
| Frequency | Percent | ||||||
| Resurgery in Iris Claw | No Resurgery | 89 | 89.0 | ||||
| Refixation | 5 | 4.0 | |||||
| Tunnel suturing | 3 | 3.0 | |||||
| Intravitreal antibiotics | 1 | 1.0 | |||||
| Reimplantation | 1 | 1.0 | |||||
| Trab + mito | 1 | 1.0 | |||||
| Total | 100 | 100.0 | |||||
| Frequency | Percent | ||||||
| Resurgery in SFIOL | No Resurgery | 98 | 98.0 | ||||
| PPV+MS + FAE+EL+SOI | 1 | 1.0 | |||||
| Vit + MP + FAE+ EL+ SOI | 1 | 1.0 | |||||
| Total | 100 | 100.0 | |||||
Mean post-operative visual acuity at 3 months was 0.68± 0.57 in Group I and 0.51± 0.36 in Group S Group S had statistically significant better visual acuity (p value- 0.016)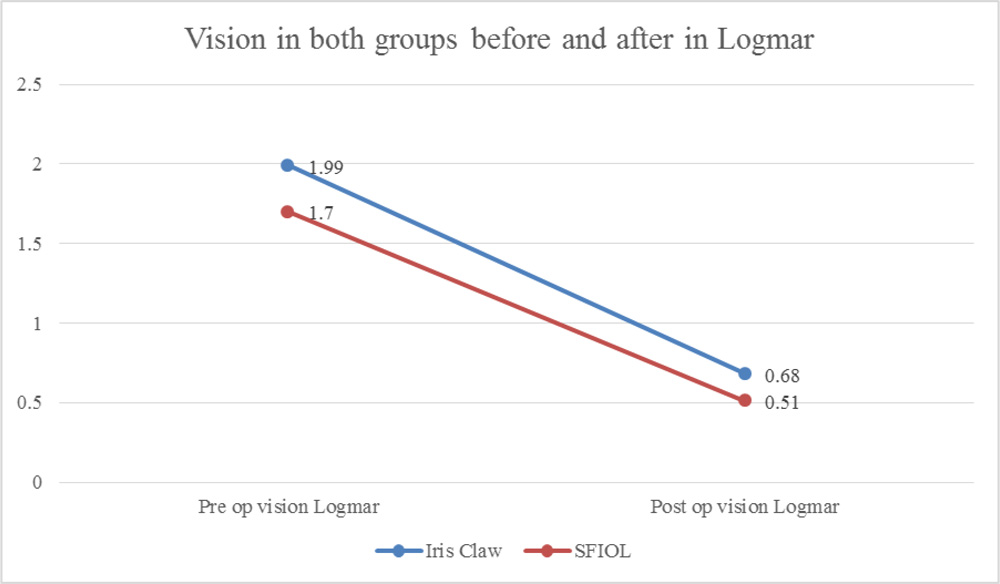
Fig 5- Comparison of pre-op and post- op vision in both groups
Discussion–
De Silva et al in 2011 reported their results of the use of anteriorly fixatediris-claw IOLs in 106 eyes. Complications included wound leak requiring re-suturing in 2.6% of eyes, postoperative intraocular pressure rise in 9.5% of eyes (glaucoma escalation 0.8%), and cystoid macular edema in 7.7% of eyes (0.8% chronic). Iris-claw IOL subluxation occurred in 6.0% of eyes from 5 days to 60 months postoperatively. In our study, Group I, one patient neededTrabeculectomy+ mitomycin C.25 eyes in our study needed re-fixation (1 needed re-implantation), 3 needed tunnel suturing comparable to De Silva’s study. We also divided our findings into complications and re-surgeries into separate groups.
Gonnerman et al reported the Artisan/Verisyse IOL implantation with posterior iris fixation in 137 eyes and achieved good visual outcomes in primary and secondary indications for implantation. Outcomes and complications compare favourably with those of alternative lOL types. Complications included slight temporary pupil ovalization in 24.8%, early postoperative hypotony in 5.1%.3 The rates of pupil ovalisation in our study were higher comparable to Gonnerman’s study. Gonnerman found cystoid macular edema in >8% eyes whereas we found CME in only 2 % patients. Patil et al reported the use of retro-fixated Iris Claw IOL in the same setting as Pars Plana vitrectomy + frag for dropped nuclear fragments and dislocated IOLs. They had a case series of 15 eyes and stated the viability of Iris claw lenses in such settings because of minimum complications and less surgical time.4
Suture- Iris Fixation and Scleral Fixation have been compared by Hara and Borkenstein and they found no complications occurred in the Iris Claw group, whereas complications were reported in seven eyes in the trans- scleral suturing fixation group throughout follow-up. They found BCVA better in Iris claw group. They also found surgical time and IOP higher in SFIOL group.5Rashad et al compared the results of retro-fixated IOL and SFIOL in 42 eyes (21 eyes in each group). They found no significant difference in vision at 3 months follow up. They found a significant IOP rise in the SFIOL group on post- operative day 1 which normalised later. Corneal edema, AC reaction and Vitreous haemorrhage were higher in SFIOL group than Iris claw group in their study. In the late period CME and IOL decentration were also higher in the SFIOL group in their study. 6
Conclusions–
To the best of our knowledge, our study has the largest sample size amongst the very few published articles comparing retro-pupillary Iris claw and scleral fixated IOL. Our study, contrary to literature, has found that SFIOLs although time consuming, is more stable in terms of visual acuity gain and lesser numbers of re-surgeries. The retrospective nature of this study is a drawback. The variable experience of the surgeons employing these two procedures also has not been accounted for. Although Iris claw IOLs are simpler to use and have lesser surgical time, using SFIOLs is a better option due to fewer re surgeries, lesser complication rate and better visual outcomes.
References
- Baykara M, Ozcetin H, Yilmaz S, Timuçin OB Posterior iris fi xation of the iris-claw intraocular lens implantation through a scleral tunnel incision. Am J Ophthalmol 2007; 144:586–591.
- De Silva SR, Arun K, Anandan M, Glover N, Patel CK, Rosen P. Iris-claw intraocular lenses to correct aphakia in the absence of capsule support. J Cataract Refract Surg 2011; 37:1667–1672.
- Gonnermann J, Klamann MK, Maier AK, Rjasanow J, Joussen AM, Bertelmann E, et al. Visual outcome and complications after posterior iris-claw aphakic intraocular lens implantation. J Cataract Refract Surg 2012; 38:2139–2143.
- Patil KB, Meleth P, Shanker MP. Pars plana vitrectomy with posterior iris claw implantation for posteriorly dislocated nucleus and intraocular lens. Indian J Ophthalmol 2011; 59:497–500.
- Hara S, Borkenstein AF, Ehmer A, Auffarth GU. Retropupillary fixation of iris-claw intraocular lens versus transscleral suturing fi xation for aphakic eyes without capsular support. J Refr act Surg 2011; 27:729–735.
- Rashad, D., Afifi, O., Elmotie, G. and Khattab, H. (2015). Retropupillary fixation of iris-claw intraocular lens versus trans-scleral suturing fixation for aphakic eyes without capsular support. Journal of the Egyptian Ophthalmological Society, 108(4), p.157.