Dr. Sumita Sethi
Gulati, S09823, Dr. Varikasuvu Seshadri Reddy,F
Dr. Ruchi Dabas, Dr. Navdeep Gupta
Authors: VS REDDY, SUMITA SETHI (Presenting author), RUCHI DABAS, NAVDEEP GUPTA.
Institute: BPS Government Medical College for Women, Khanpur Kalan, Sonepat, Haryana
Abstract:
To investigate the status of oxidative stress by plasma total antioxidant capacity (TAC) and aqueous humor ischemia modified albumin (IMA) levels in patients with senile cataracts. 63 senile cataract and 50 healthy controls included.
TAC measured by ferric reducing ability of plasma before and within 24 hours post-surgery; aqueous humor IMA measured by nickel albumin binding assay. In aqueous humor, we could not detect IMA levels in randomly chosen 11 samples (Mean±SE 0.03±0.006, Median 0.02 ABU).
A significant decrease (p<0.05) in TAC in cataracts patients (0.97±0.44) compared to controls (1.76±0.32 mmol/L). No significant difference in TAC levels pre and post-surgery. TAC level better distinguishes the status of oxidative stress between controls and cataracts (criterion ≤1.4 mmol/L, sensitivity 88.9, specificity 90.0, and AUC 0.90). Significant decrease in the levels of TAC which remains decreased after surgical treatment in cataract suggests the need for antioxidant supplements.
Introduction:
Senile cataract is a leading cause of blindness and low vision worldwide. It is estimated that 44.1% of blind patients and 51.6% of patients with low vision have cataract.1 In developing countries, 50–90% of all blindness is caused by cataracts.2 The development of cataract is a multifactorial process and several factors such as genetic, gender, geographic location, ultraviolet light exposure, systemic diseases like diabetes, level of education, occupation and nutrition have been found to be associated with cataract formation. Universally age is the most important risk factor and about 85 per cent of patients have senile cataract.3 Since senile cataract cannot be prevented from occurring there has been an interest in understanding of factors that can slow down the development of the cataracts. It has been estimated that a delay in cataract formation for 10 years will reduce the prevalence of the cataracts by 50%.4
It has been accepted that pathogenesis of cataract is influenced by a number of biochemical factors including oxidative stress.4-8 Oxidative stress results of a dyshomeostasis between pro-oxidants and antioxidants. It is an imbalance between the production of various reactive species and the ability of the natural protective mechanisms in the body to cope with these reactive compounds and prevent adverse effects. The study was undertaken to investigate the status of oxidative stress by plasma total antioxidant capacity (TAC) and aqueous humor ischemia modified albumin (IMA) levels in patients with senile cataracts.
METHODOLOGY:
Subjects:
We conducted a prospective, case-controlled study of 63 patients with senile cataracts and 50 healthy controls. Subjects with clinical diagnosis of senile cataract were included after undertaking complete ophthalmic work-up. The diagnosis of cataract was based on biomicroscopy evaluation. Age and sex matched controls were recruited among patients who attended the hospital during the same period for other ocular problems like refractive errors. During selection of cases and controls, it was made sure that they were free from any chronic disease or metabolic disorder. Also those with steroid use or who smoked cigarettes were not included. The procedure was explained to them and written informed consent was taken to participate in the study.
Blood collection:
Venous peripheral blood samples were collected after 12 hour overnight fasting from each subject at the time of admission and within 24 hours after surgery.
Aqueous collection:
Aqueous (0.5-1.0 ml) was collected at the beginning of the surgery through paracentesis under fill aseptic precautions (only in cases).
Laboratory analysis:
Biochemical analysis was performed immediately / same day. TAC was evaluated by Ferric reducing ability of plasma (FRAP); aqueous humor IMA levels by nickel albumin binding assay.
Statistical Analysis:
MEDCALC; ANOVA, Correlations and ROC were used for statistical analysis. P-value of ≤0.05 was considered significant.
RESULTS:
We observed a significant decrease (p<0.05) in TAC in cataract patients (0.97±0.44) compared to controls (1.76±0.32 mmol/L) (table-1). No significant difference in TAC levels was detected between pre and post-surgery samples of cataract patients and with duration of disease (figure-1,2). Receiver operating curve (ROC) analysis showed that the TAC level better distinguishes the status of oxidative stress between controls and cataracts (criterion ≤1.4 mmol/L, sensitivity 88.9, specificity 90.0, and AUC 0.90) (figure-3). In aqueous humor, we could not detect IMA levels in randomly chosen 11 samples (Mean±SE 0.03±0.006, Median 0.02 ABU).
Table-1: TAC levels before and after surgery
| Variable | CASES | CONTROLS | |
| Before surgery | After surgery | ||
| Age | 61.9±11.2 | 61.9±11.2 | 57.7±9.2 |
| Sex (m/f) | 39/24 | 39/24 | 30/20 |
| TAC (mmol/L) | 0.97±0.44* | 1.04±0.45* | 1.76±0.32 |
Figure-1: TAC levels before and after surger
Figure-2: TAC levels in relation to duration of disease 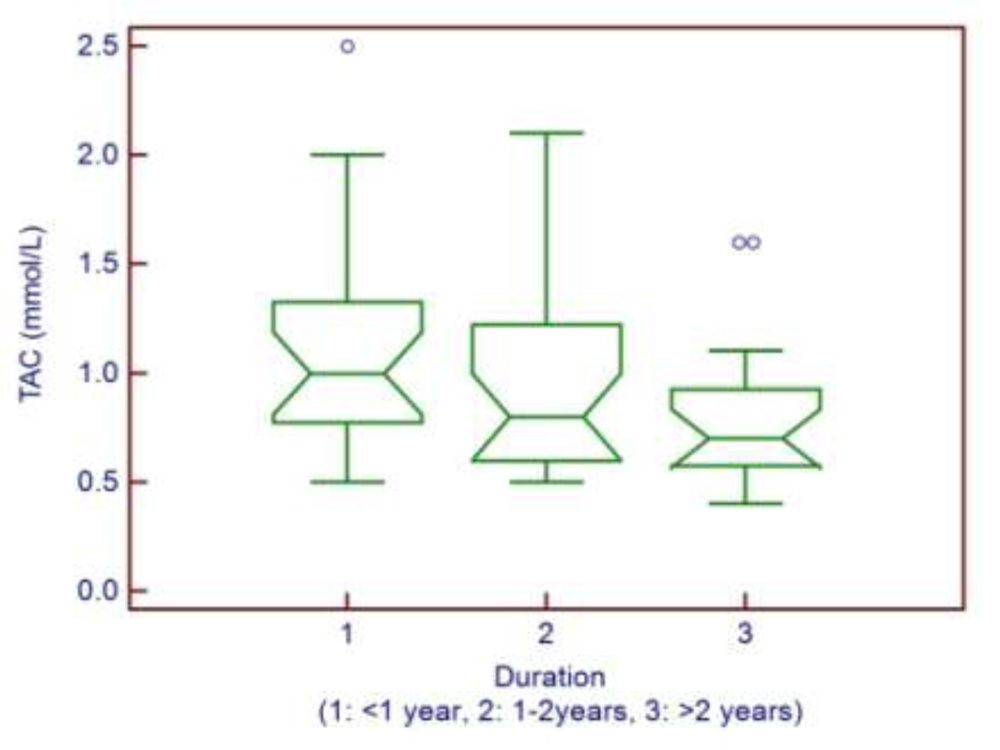
Figure-3: Receiver operating curve (ROC) analysis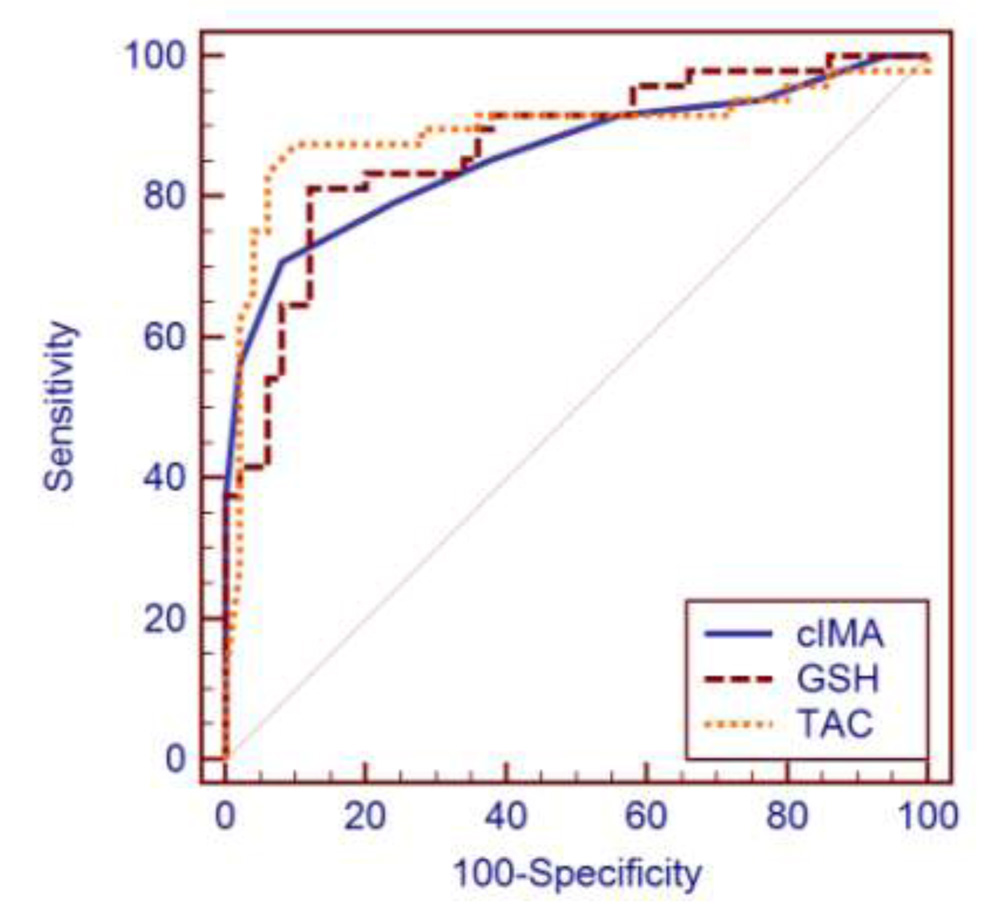
DISCUSSION:
‘VISION 2020:The Right to Sight’, launched in 1999 by the World Health Organization (WHO) and the International Agency for the Prevention of Blindness (IAPB), aims to reduce preventable blindness by the year 2020. Detection and elimination of blindness-causing diseases and related risk factors is a priority of the program and cataract as the major reason of blindness is a major concern.9 There has been recent interest in understanding of oxidative stress as a major biochemical mechanism underlying cataractogenesis and the role of antioxidative capacity as a preventable factor in development of cataract. Although there are multiple physiologic defence mechanisms to protect the lens from the toxic effects of oxidative damage, there is increasing evidence which suggests that to oxidative stress over the long-term may predispose the lens to cataract development.10
We utilized plasma TAC as an indicator for oxidative stress in cataract patients. While the level of TAC decreased within 24 hours after cataract surgery, it was not statistically significant. However in comparison with the control group, level of TAC was significantly less in cataract patients both before and after surgery. There was no significant correlation with duration and type of cataract.
Vîrgolici B et al. put forward an interesting hypothesis that senile cataract is a systemic disease with an inflammatory component, they demonstrated that cataract formation is due to primary role of systemic oxidative stress generated outside the lens.11 Abraham Spector had a remarkable observation that the epithelial cell layer is the initial site of attack by oxidative stress which is followed by involvement of the lens fibers, leading to cortical cataract.12 Li L at al concluded that subjects with early onset cataract are under increasing systemic oxidative stress.7 Our findings were in accordance with Chang D et al. who found a significant decrease in antioxidative enzymes and increase in oxidative stress products in cataract patients in comparison to the control subjects.8 Studies taking into account cataract in diabetic patients have concluded that diabetic patients are subjected to more oxidative stress at a much earlier age as compared to senile cataract patients.6
There are not many studies on oxidative stress markers in human aqueous humor. Most of the studies which have measured IMA in various body fluids have utilized Cobalt binding assay;13,14 recent evidence have indicated that Nickel binding is a more efficient and discriminate assay. We have made use of Nickel binding assay for IMA detection in the aqueous. W. Russell McLauchlan et al. investigated the suitability of the Total Antioxidant Activity (TAA) assay to measure the total antioxidant activity of human aqueous humor and concluded that human aqueous humor follows lag phase kinetics consistent with aqueous acting as a sacrificial antioxidant.15 In our study we could not detect IMA levels in randomly chosen 11 aqueous samples (Mean±SE 0.03±0.006, Median 0.02 ABU). Though no explicit explanation can be provided, this could probably be attributed to less number of samples.
It remains a topic of debate as to whether the modified oxidative stress markers are cause or effect in senile cataract. Our results of significant decreased levels of TAC which remains to be decreased after surgical treatment in cataract suggest and support the involvement of oxidative stress in cataract. Our findings strongly support the need for direct antioxidant supplementation in these patients.
References:
1.Resnikoff S, Pascolini D, Etya’ale D, Kocur I, Pararajasegaram R, Pokharel GP et al. Global data on visual impairment in the year 2002. Bull World Health Organ 2004; 82: 844–51.
2.Robinson B, Acorn CJ, Millar CC, Lyle WM. The prevalence of selected ocular diseases and conditions. Optom Vis Sci 1997; 74: 79–91.
3.west SK, Valmadrid CT. Epidemiology of risk factors for age-related cataract. Surv Ophthalmol 1995; 39: 323–34.
4.HARDING J.J., Physiology, biochemistry, pathogenesis, and epidemiology of cataract. Current Opinion in Ophthalmolology, 1992; 3:3–12.
5.Kisic B, Miric D, Zoric L, Ilic A, Dragojevic I. Antioxidant capacity of lenses with age-related cataract. Oxid Med Cell Longev. 2012;2012:467130.
6.Katta AV, Katkam RV, Geetha H. Lipid peroxidation and the total antioxidant status in the pathogenesis of age related and diabetic cataracts: a study on the lens and blood. J Clin Diagn Res. 2013 Jun;7(6):978-81.
7.Li L, Duker JS, Yoshida Y, Niki E, Rasmussen H, Russell RM, Yeum KJ. Oxidative stress and antioxidant status in older adults with early cataract. Eye (Lond).2009 Jun;23(6):1464-8.
8.Chang D, Zhang X, Rong S, Sha Q, Liu P, Han T, Pan H. Serum antioxidative enzymes levels and oxidative stress products in age-related cataract patients. Oxid Med Cell Longev. 2013;2013:587826.
9.Resnikoff S, Pararajasegaram R. Blindness prevention programmes: pas t, present, and future. Bull World Health Organ 2001; 79: 222–6.
10. GUL A., RAHMAN M.A., HASNAIN S.N., SALIM A., SIMJEE S.U., Could Oxidative Stress Associate with Age Products in Cataractogenesis? Curr. Eye Res., 2008, 33(8):669–75.
11.Vîrgolici B, Stoian I, Muscurel C, Mărăcine M, Popescu L, Moraru C, Dinu V. Systemic redox modifications in senile cataract. Rom J Intern Med. 2009;47(3):279-87.
12.Spector A. Oxidative stress-induced cataract: mechanism of action. FASEB J 1995;9:1173–82.
13.Mothes E, Faller P. Evidence that the principal CoII-binding site in human serum albumin is not at the N-terminus: implication on the albumin cobalt binding test for detecting myocardial ischemia. Biochemistry. 2007 Feb 27;46(8):2267-74.
14.Koc F, Erdem S, Altunkaş F, Ozbek K, Gül EE, Kurban S, Taşyürek E, Erbay E, Söğüt E (2011). Ischemia-modified albumin and total antioxidant status in patients with slow coronary flow: a pilot observational study. Anadolu Kardiyol Derg; 11:582-7.
15. Russell McLauchlan, Julie Sanderson, Michael Quinlan, Gary Williamson. Measurement of the Total Antioxidant Activity of Human Aqueous Humor. Clinical Chemistry 1998;44 (4): 888-889.