Dr. Liya Susan Peter, P18548 Dr. Suneetha N Lobo, Dr. Mary Joseph, Dr.Sangeetha Sriram
ABSTRACT :
Aim:
In this study we evaluated outcome of rhino-orbital mucormycosis treated at our hospital.
Method:
Retrospective case series of 34 patients with ROM.All patients were treated with IV amphotericin-B.
Results:Uncontrolled diabetes was predisposing factor in all. Orbital involvement presented with ptosis,proptosis,EOMrestriction,RAPD and CRAO.Cerebral involvement in 12, 5 deaths due to intracranial spread,17 patients discharged with suboptimal therapy.Improvement in orbital signs alone seen in 4/12,no improvement in 4/12, improvement in orbital signs and vision in 4/12 who also received posaconazole.
Conclusion:All patients who completed antifungal therapy had good outcomes. Addition of posaconazole reduced morbidity.Financial constraints is an important hurdle for treatment.
INTRODUCTION:
Invasive fungal infections have increased over the past few years, especially in immunocompromisedpatients.1Mucormycosis is an invasive fungal infection caused by filamentous fungi belonging to the Mucoraceae family. It is subdivided into three genera Absidia, Rhizopus and Rhizomucor [Mucor].1, 2It is a life threatening disease associated with severe morbidity and mortality.Diabetes mellitus with or without ketoacidosis and immunosuppression are important predisposing factors for the same.3, 4
The paucity of therapeutic options magnifies the challenge of treating this disease.5Combinedtreatment of surgical debridement with prolonged high-dose liposomal amphotericin B is the treatment of choice as there is a high risk of treatmentfailure when antifungals are used in isolation.Posaconazole,a triazole antifungal, is used as salvage therapy.6,7
METHOD:
This is a retrospective study on 34 patients with a histopathological diagnosis of Rhino Orbital Mucormycosis [ROM] who were admitted in a tertiary hospital from 2012-2016. In this study we evaluated the outcome of ROM treated at our hospital.
Medical records were analysed and demographic details including age and gender was noted.Clinical information such as visual acuity, presence of ptosis and proptosis, pupillary reaction, presence of Relative Afferent Pupillary Defect [RAPD], features of Central Retinal Artery Occlusion [CRAO] on fundus examination and extra ocular movements [EOMS] at the time of admission and at discharge were noted.
Random blood sugar [RBS] value at the time of admission, presence of any predisposing factors, medical and surgical treatment, treatment outcome and availability to follow up were also noted.
All patients were treated with IV amphotericin-B. 31/34[91.17%] underwent paranasal sinus debridement. Exentration was done in 2/34[5.88%] and 4 received oral posaconazole as salvage therapy.
STATISTICAL ANALYSIS:
Descriptive statistics including mean with standard deviation for continuous variables and frequency counts with percentages were computed.
RESULTS:
The details of 34 patients of ROM were complete and included for analysis.
Patient population comprised of 34 patients (24males and 10 females) between the age group of 25 to 84 years with a mean age of 52.38+/-13.[Table1].Uncontrolled diabetes with and without ketoacidosis was a predisposing factor in all our patients. Average RBS was found to be 340.5 +/- 91.24 ranging from 208 mg/dl to 600 mg/dl. Ketoacidosis was found in 5 people.
All patients had orbital involvement, characterized by ptosis, proptosis, EOMS restriction, RAPD and CRAO. [Table 2]
Cerebral involvement was noted in 12/34[35.29%] of which 5 patients were not oriented to time, place and person.There were 5 deaths due to intracranial spread.Average GCS at admission was 5. Reasons for death includecerebral infarcts, cerebellar infarct, internal carotid artery occlusions, bilateral spontaneous extra duralhemorrhage and coagulopathy with multiple intracranialhemorrhages. [Table 3]
17/34[50%] patients got discharged after receiving suboptimal antifungal therapy. Nine of them got discharged against medical advice within 2 weeks of admission, 6 of which were due to financial constraints and remaining 3 due to long duration of stay at hospital and preferred going to an institute closer to their residential area. 8 patients got discharged within 2-4 weeks of treatment of which 6 were due to financial constraints and 2 were due to dissatisfaction to treatment response despite a long stay at hospital. [Table 3]
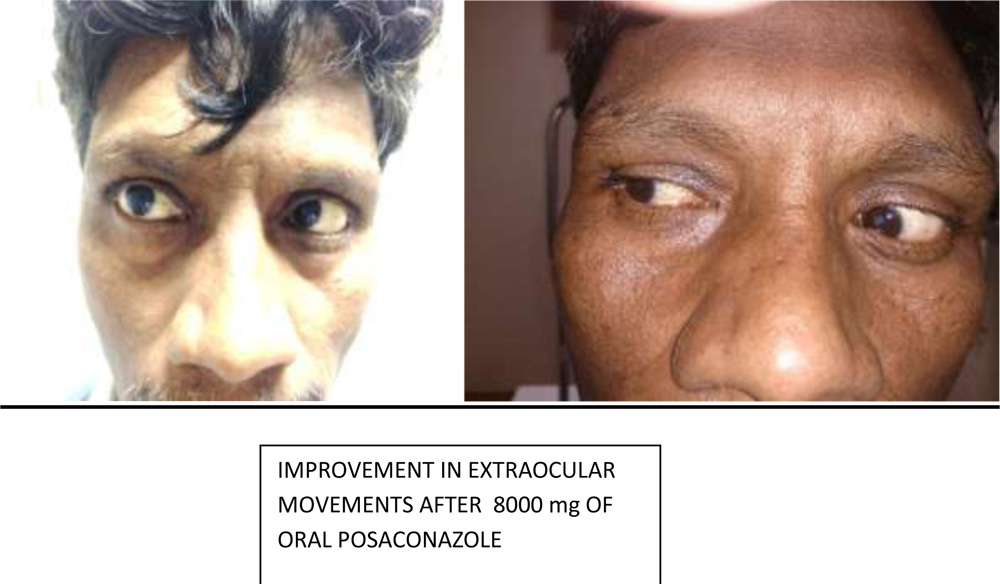
Only twelve patients were available for 1-2 months follow up.Among these improvement in orbital signs with no improvement in vision was seen in 4/12[33.33%]. No improvement was noted in orbital signs and vision in 4/12[33.33%]. Improvement in both orbital signs and vision occurred in 4/12[33.33%],all of whom had received posaconazole in addition to amphotericin B. [Table 3]
DISCUSSION :
Mucormycoses are omnipresent saprophytes which are found in the nose, mouth and throats of healthy individuals. These fungi gain access to the oral and nasal mucosa by inhalation of the air borne spores produced by them.The endothelium of the blood vessels is damaged due to angioinvasion which results in the development of a thrombus leading to ischemia and infarction of the tissues. This leads to the characteristic black necrotic eschar of the skin and mucosa. Fungal growth flourishes in the acidotic environment formed due to ischaemia. The poor vascular supply hinders the eradication of the fungus by systemic anti-fungal agents.2
The most common and lethal presentation of mucormycosis is Rhino Oculo Cerebral Mucomycosiswhich is an acute and fulminant infection that originates in the nasal cavity and rapidly invades the paranasal sinuses and orbit and eventually involves the intracranial structures either by angioinvasion or by direct extension through the orbital apex.Diabetics are predisposed to mucormycosis because of the decreasedability of their neutrophils to phagocytize and adhere to endothelial walls.2 High blood sugar level may also alter theability of macrophages.8As the underlying medical condition is manageable, diabetics have the best chance of survival.2In our study, all 34 patients had uncontrolled blood sugars.
Common signs and symptoms include headache, unilateral facial pain and swelling, acute sinusitis, unilateral periorbital swelling, decreased vision, necrotic ulcer in the nasal or oral mucosa and alterations in mental state. Patient can present with the orbital apex syndrome characterised by ptosis, proptosis, ophthalmoplegia, sensory deficitand visual loss may be the initial manifestation of thedisease.9
Progressive involvement of the central nervous system is found to be fatal.3In our study, 5 cases with CNS involvement succumbed to the infection.
Treatment strategies include aggressive surgical debridement of involved tissue, antifungal agents, prompt control of hyperglycemia and increasing patients immunity.2,3
Blood vessel thrombosis with resulting tissue necrosisleads to poor penetration of systemic antifungal agents to the site of infection. Hence, debridement of devitalized tissues is necessary for complete eradication of mucormycosis.6 Thirty onepatients included in our study underwent paranasal sinus debridement.
Parenteral polyene-based (amphotericin B) therapy is the treatment of choice.[3] All our patients received amphotericin B. Of the 12 patients available for follow up, 8 patients received a cumulative dose of >1500 mg of amphotericin B. Four of these showed improvement in orbital signs. However, none of them showed improvement in vision. Four showed no improvement in orbital signs or in vision.
Compared to antifungal therapy alone, survival chances are seen more with a combined medical and surgical approach. 5,6,7
Posaconazole therapy can be considered in refractory cases or in patients who are intolerant to polyenes. 3Van Buriket al.10 reported that 60% showed good response (15% complete response, 45% partial response) to posaconazole when used as salvage therapy. Greenberg et al.11 also noted similar results. It is dosed at 400 mg twice daily.
We found out that 4 of our patients who were not responding to amphotericin B, showed improvement in both orbital signs and vision after the administration of oral posaconazole. All 4 received a cumulative dose of >8000 mg of posaconazole. One patient who received inadequate posaconazole therapyof 1800 mg showed no improvement.
Half the number of patients received sub optimal treatment. Few preferred to continue treatment in a local hospital near to their residential area. Two got discharged against medical advice due to dissatisfaction at treatment response
CONCLUSION :
Patients with mucormycosis have lesser mortality and morbidity if they have completed the course of amphotericin B with strict control of diabetes. Salvage therapy with posaconazole shows promise in patients who fail to respond to amphotericin B. However due to the financial constraints or delay in improvement of symptoms patients in our scenario fail to complete treatment and are lost to follow up.
REFERENCES :
1. Nitin MN, Hitesh V, Rps P. Co-existing Mucormycosis with Aspergillosis in a patient with Diabetes Mellitus-First case report. Online Journal of Otolaryngology. 2014 Oct
2.Songu M, Unlu HH, Gunhan K, Ilker SS, Nese N. Orbital exenteration: a dilemma in mucormycosis presented with orbital apex syndrome. American journal of rhinology. 2008 Jan 1;22:98-103.
3.Rath B, Samant M, Swain KP, Mallick AK. Rhino-oculocerebral Mucormycosis. Annals of Tropical Medicine and Public Health. 2015 Sep 1;8:214.
4.Ribeiro LC, Wanke B, Da Silva M, Dias LB, Mello R, Canavarros FA, Leite-Jr DP, Hahn RC. Mucormycosis in MatoGrosso, Brazil: a case reports, caused by Rhizopusmicrosporus var. oligosporus and Rhizopusmicrosporus var. rhizopodiformis. Mycopathologia. 2012 Mar 1;173:187-92.
5.Gamaletsou MN, Sipsas NV, Roilides E, Walsh TJ. Rhino-orbital-cerebral mucormycosis. Current infectious disease reports. 2012 Aug 1;14:423-34.
6.Spellberg B, Ibrahim AS. Recent advances in the treatment of mucormycosis. Current infectious disease reports. 2010 Nov 1;12:423-9.
7.Kulendra K, Habibi M, Butler C, Clarke P, Howard D. Use of posaconazole in the treatment of infective rhinocerebral mucormycosis. The Journal of Laryngology & Otology. 2010 Dec 1;124:1314-7.
8.Mohammadi R, Nazeri M, Sayedayn SM, Ehteram H. A successful treatment of rhinocerebral mucormycosis due to Rhizopusoryzae. Journal of research in medical sciences: the official journal of Isfahan University of Medical Sciences. 2014 Jan;19:72.
9.Rahman A, Akter K, Hossain S, Rashid HU. Rhino-orbital mucourmycosis in a non-immunocompromised patient. BMJ case reports. 2013 Feb 7;2013:bcr2012007863.
10.vanBurik JA, Hare RS, Solomon HF, Corrado ML, Kontoyiannis DP. Posaconazole is effective as salvage therapy in zygomycosis: a retrospective summary of 91 cases. Clinical Infectious Diseases. 2006 Apr 1;42:e61-5.
11.Greenberg RN, Mullane K, Van Burik JA, Raad I, Abzug MJ, Anstead G, Herbrecht R, Langston A, Marr KA, Schiller G, Schuster M. Posaconazole as salvage therapy for zygomycosis. Antimicrobial Agents and Chemotherapy. 2006 Jan 1;50:126-33.
Table 1: BASELINE DEMOGRAPHIC CHARACTERISTICS:
| Sl No: | Variable | Number [%] |
| 1. | Mean age +/- SD | 52.94+/-13.29 |
| 2. | Gender
Males Females |
24 [70.50%] 10 [29.41%] |
Table 2:DESCRIPTIVE STATISTICS OF THE VARIABLES:
| Sl. No: | Variable | Number [%] |
| 1. | Ptosis
Present Absent |
12 [35.29%] 22 [64.70%] |
| 2. | Proptosis
Present Absent |
14 [41.17%] 20 [58.82%] |
| 3. | Pupillary reaction
Brisk Sluggish Non-reactive |
06 [17.64%] 18 [52.94%] 10 [29.41%] |
| 4. | RAPD
Present Absent |
05 [14.70%] 29 [85.29%] |
| 5. | CRAO
Present Absent |
04 [11.76%] 30 [88.23%] |
| 6. | Extra ocular movements
Normal Restricted Total ophthalmoplegia |
06 [17.64%] 22 [64.70%] 06 [17.64%] |
Table 3: DESCRIPTIVE STATISTICS OF TREATMENT OUTCOME:
| Sl. No: | Variable | Number |
| 1. | No improvement in orbital signs & vision | 04 |
| 2. | Improvement in orbital signs alone | 04
|
| 3. | Improvement in both orbital signs and vision | 04 |
| 4. | Discharged against medical advice
|
17 |
| 5. | Dead
|
05 |